The plan was to begin handing out boxes of groceries at 11, but the Facing Hunger Foodbank truck delivering the food blew a tire en route. No one complained.
Perry Hall was among those waiting. His wife, Lilly Hall, volunteers with the distribution team. Perry has been dealing with a form of cancer called multiple myeloma. The Halls get by on around $1,500 a month from his Social Security benefits, plus assistance from the federal Supplemental Nutrition Assistance Program, or SNAP. But because of her age, Lilly, 59, recently became subject to new SNAP work requirements and at risk of losing her benefits.
As part of the federal One Big Beautiful Bill Act, all “able-bodied adults” 64 or younger who don’t have dependents and don’t work, volunteer, or participate in job training at least 80 hours a month are now restricted to three months of benefits every three years from SNAP, formerly known as food stamps. Previously, the federal requirement applied to those 54 or younger. The new rule, which went into effect in November, also applies to parents of children 14 or older. And it removed exemptions for veterans, people experiencing homelessness, and young adults who’ve aged out of foster care.
Proponents of work requirements argue that they incentivize people who are “work-ready” to seek and keep jobs, reducing dependence on government assistance and upholding the “dignity of work.”
Rhonda Rogombé serves as health and safety net policy analyst for the West Virginia Center on Budget and Policy. She and her colleagues have studied the effects of SNAP work rules and found that requiring recipients to work does not lower an area’s unemployment rate.
Previous work requirements were suspended nationwide during the covid pandemic and reinstated in fall 2023. The researchers found that the average number of people employed in Mingo County each month actually went down after the requirement was reimposed.
A 2018 federal research project that examined several data sources, including SNAP data from nine states, found that work requirements “have no impact on labor force participation and the number of hours worked.”
There are a number of possible explanations, Rogombé said, “but when people are hungry, they’re not able to support themselves. When people are hungry, it’s harder to focus at work. It’s harder to engage in work activity, and we think that that’s part of it.”
Jobs are scarce in this southern West Virginia county. Lilly Hall found work at a Delbarton restaurant. But it’s unpaid until a waitress position opens — enough to preserve her benefits, but far from ideal.
On that mild Wednesday in late March, House of Hope provided chicken, eggs, bread, potatoes, fresh fruit and vegetables, and milk.
Among those in line were older residents and “some young people that have lost their way and they can’t get work and they just need help,” said Timothy Treleven, who operates the pantry with his wife, Christine, and Gail Lendearo.

House of Hope’s scheduled distribution day is the last Saturday of each month — supplemented by occasional weekday Facing Hunger visits — as money from monthly checks begins to run out and cupboards go bare.
On a typical Saturday, pantry staff and volunteers hand out up to 400 boxes of food.
“It’s an honor to do this,” Lendearo said. “It’s a blessing.”
Perry Hall’s cancer is now in remission, but for a while his treatment required that he and Lilly travel back and forth, 4½ hours each way, to Morgantown. The couple’s van couldn’t make the trip, so they paid a friend for rides.
Mingo’s population is just under 22,000, down from around 27,000 in 2010. It once flourished, fueled by coal. Williamson, the county seat, was home to an opera house and businesses operated by immigrants from Italy, Russia, and Syria. The region is still referred to as “the coalfields,” but little is mined here these days. A quarter of residents live in poverty.
Rogombé and her colleagues found that Mingo County residents face significant barriers to securing what few jobs are available. These include unreported physical and mental impairments, housing insecurity, and a lack of high school diplomas and identification documents.

Filing the paperwork to receive benefits or to confirm compliance is difficult for many residents. The West Virginia Center on Budget and Policy’s research found that about 1 in 4 lack reliable internet access.
Additional changes lie ahead for the SNAP program. Currently, the federal government and the states share administrative costs equally, but in October states will assume 75% of those costs. And beginning in October 2027, they’ll be required to pay additional costs based on error rates.
Kentucky, like West Virginia, is among the poorer states that will be most affected by the new requirements and costs. The Kentucky Center for Economic Policy estimates that up to 114,000 residents risk losing SNAP benefits with the expanded work requirements.
Jessica Klein, a researcher with the center, worries about the consequences. “We know SNAP has an impact on health, and not just because it decreases food insecurity,” she said. It worsens blood pressure rates, obesity, medication adherence, and more.
With the additional financial burden placed on states, “I think what we’ll see is some states changing rules that impact participation in order to have a smaller, more affordable program,” Klein said. “My fear is that some states will choose not to operate SNAP at all.”
In Mingo County, folks are stepping up. At least eight food pantries offer groceries to those in need.
Janet Gibson runs the Blessing Barn pantry in the Ben Creek community. “I can go from one end of the creek to the other” and tell you everyone’s name and a little something about them, she said. She takes pride in feeding her people.

Gibson said it can be hard to find even volunteer opportunities in the county, largely because of transportation challenges. A look at a local map can be misleading: A couple of dozen miles into a holler or up a ridge could take an hour or more.
“Whether you’re working full-time or not, you’re still spinning out gas to get to work,” Gibson said, “and gas ain’t cheap now.”
A single mother of three, Trista Shankle of Paducah, Kentucky, isn’t subject to the new SNAP requirements, but she worries about the fragility of the social safety net. She overcame challenges, is earning a master’s degree in social work, and works for an organization that connects community college students with Temporary Assistance for Needy Families benefits. Her family receives SNAP, Medicaid, housing support, and assistance from the USDA’s Special Supplemental Nutrition Program for Women, Infants, and Children. If any one of those is cut, she said, she may have to drop out of school.
Shankle is certain she wouldn’t have advanced to where she is today without the benefits she and her family have received: “They bring a sense of calm and comfort. I know that my kids aren’t going to go hungry.”
The first week in April, Lilly Hall reported for work at Black Bear Trails Restaurant. She’s grateful for the opportunity. And when a waitress slot opens, “I’ll snag that position so quick it’ll make your head flip.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.This <a target="_blank" href="https://kffhealthnews.org/medicaid/food-stamps-snap-work-requirements-hunger-west-virginia-foodbanks/">article</a> first appeared on <a target="_blank" href="https://kffhealthnews.org">KFF Health News</a> and is republished here under a <a target="_blank" href="https://creativecommons.org/licenses/by-nc-nd/4.0/">Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="https://kffhealthnews.org/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="https://kffhealthnews.org/?republication-pixel=true&post=2228111&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>{kind=link}
But officials warned that all optional Medicaid services are still under review as the state health department looks for cuts to offset a shortfall driven by higher-than-expected Medicaid costs.
Jon Ebelt, a spokesperson with the Montana Department of Public Health and Human Services, said the agency is preparing a request to the federal government to add doula care to the state’s Medicaid program. It would cost the state about $118,000 in its first year to provide doula Medicaid reimbursements, according to state estimates.
His April 15 comments came three weeks after department officials told KFF Health News that the state budget deficit had put those plans on hold. Ebelt denied that a final decision had been made in March to scrap the doula Medicaid payments, which state lawmakers approved in a bill last year. The coverage is “now proceeding as planned,” he said.
“At the time of your initial inquiry, we were still in the process of analyzing the appropriation,” Ebelt said.
Federal health officials must approve any amendments to the state’s Medicaid program before payments can begin. At least 25 other states reimburse doulas through Medicaid.
Doulas are trained, nonmedical workers who support people through pregnancy and after they give birth. The care they provide is linked to reductions in health complications, which has prompted more states to cover doula services in recent years.
Montana lawmakers who supported expanding Medicaid to cover doula care in 2025 cited scarce maternity services, especially in rural and Indigenous communities. But this year, the state has a Medicaid budget deficit of more than $177 million and is expecting a similar shortfall next year. Plus, federal policy changes slated to take effect later this year are expected to increase costs.
“ There’s a need and a desire for doula services, but a lot of people can’t afford it,” said Sheri Walker, a Helena-based doula and president of the Montana Doula Collaborative. “So that means many of us have other jobs that we have to juggle.”
Walker is a part-time labor and delivery nurse outside of her doula work.
On March 25, health department spokesperson Holly Matkin said in an email to KFF Health News that the agency “will not be moving forward with the implementation of doula services in the Montana Medicaid benefit package at this time.” She had added that it was unclear whether state law gives the department the authority to authorize coverage during the budget shortfall.
State Sen. Cora Neumann, a Democrat who sponsored last year’s bipartisan doula reimbursement bill, said she didn’t know about the department’s plans until she saw KFF Health News’ reporting. Neumann said she and groups that had backed the legislation began calling health officials, making the case for doula services as a low-cost way to provide critical care.
After about a week, Neumann said, state officials told her the agency was moving ahead with doula services after all.
“They were on the chopping block,” Neumann said. “This is a story of how important it is for all Montanans to pay attention and stay connected to what’s happening.”
Ebelt did not clarify what led the department to change its position. However, he warned that optional Medicaid services, such as doula services, may still be cut.
“All optional services, including this service, are being reviewed,” Ebelt said, referring to doula care. He did not respond to a follow-up query as to whether the department might still decide to postpone the program following federal approval.
Optional services are types of care that states choose to cover through their Medicaid programs but aren’t required by federal law. That can include covering eyeglasses, prescription drugs, and prosthetics, and more specialized care such as physical therapy, or inpatient psychiatric services for people under 21.
Those services may not sound optional, said Liz Williams, who studies Medicaid financing at KFF, a health information nonprofit that includes KFF Health News. But she said they’re one of the few avenues states have to make adjustments when budgets get tight.
Congressional Republicans’ One Big Beautiful Bill Act, the spending measure President Donald Trump signed into law last July, is expected to put more states in a budget crunch as its provisions start to take effect by the end of the year. The federal government has estimated that the law will reduce federal Medicaid spending by nearly $1 trillion over 10 years. The law also left states with a higher share of the costs to provide food assistance.
Williams said many states expanded services in recent years by boosting optional Medicaid benefits and provider pay.
“We could see them walk those back,” Williams said.
Montana’s financial problems preceded federal changes. Last year, state lawmakers cut some of the health department’s funding and underestimated Medicaid use. The state also overestimated what the federal government would pay toward Montana’s Medicaid costs.
Health officials must outline a plan to cut costs before the state’s 2027 budget year begins on July 1. Simultaneously, the agency is trying to hire more staffers to begin vetting whether Medicaid enrollees meet or are exempt from new work requirements that also go in place July 1. The new rules, mandated through long-delayed state legislation and the federal spending law, will have a three-month grace period.
Stephanie Morton, executive director of Healthy Mothers, Healthy Babies-The Montana Coalition, said she’s grateful the state is back on track to pay for doula services through Medicaid. But she said she’s worried about potential health care cuts to come.
“We know that doulas are a critical piece of that infrastructure, but standing alone and losing other sources of care really isn’t optimal,” Morton said. “These are not robust systems as it stands.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.This <a target="_blank" href="https://kffhealthnews.org/medicaid/doula-care-pregnancy-medicaid-montana-budget-cuts/">article</a> first appeared on <a target="_blank" href="https://kffhealthnews.org">KFF Health News</a> and is republished here under a <a target="_blank" href="https://creativecommons.org/licenses/by-nc-nd/4.0/">Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="https://kffhealthnews.org/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="https://kffhealthnews.org/?republication-pixel=true&post=2229052&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>
KFF Health News Michigan correspondent Kate Wells discussed urgent care clinics offering abortions on Apple News Today on April 15.
- Click here to hear Wells on Apple News Today.
- Read Wells’ “Urgent Care Clinics Move To Fill Abortion Care Gaps in Rural Areas.”
KFF Health News Montana correspondent Katheryn Houghton discussed doula Medicaid reimbursements on Montana Public Radio on April 9.
- Click here to hear Houghton on Montana Public Radio.
- Read Houghton’s “This Northern Cheyenne Doula Was About To Start Getting Paid — Then Medicaid Cuts Hit.”
KFF Health News contributor Michelle Andrews discussed farm bureau health plans on The Yonder Report on April 8.
- Click here to hear Andrews on The Yonder Report.
- Read Andrews’ “Farm Bureau Health Plans Beat the ACA on Prices With an Age-Old Tactic: Rejecting Sick People.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
This <a target="_blank" href="https://kffhealthnews.org/on-air/on-air-april-18-2026-urgent-care-abortion-doulas-farm-bureau-health-plans/">article</a> first appeared on <a target="_blank" href="https://kffhealthnews.org">KFF Health News</a> and is republished here under a <a target="_blank" href="https://creativecommons.org/licenses/by-nc-nd/4.0/">Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="https://kffhealthnews.org/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="https://kffhealthnews.org/?republication-pixel=true&post=2183401&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>But Republican lawmakers in some states think the new rules — part of the GOP’s One Big Beautiful Bill Act, signed last July by President Donald Trump — don’t go far enough.
Indiana is leading that charge, with a new law that requires applicants to prove they’ve been working or participating in a similar activity for three consecutive months to get benefits.
Meanwhile, residents in many other states will have to show they’ve been working just one month, the least cumbersome option under Trump’s signature tax-and-domestic-spending law. It instructs states to decide whether to require one, two, or three months of work history.
As in Indiana, Republican Idaho lawmakers approved a three-month requirement, and the state’s governor signed the bill into law on April 10.
The efforts, along with similar moves in Arizona, Missouri, and Kentucky, are aimed at restricting flexibility to implement the federal law at the state level.
“Normally, you would not see state legislators weighing in on these decisions,” said Lucy Dagneau, a senior official with the American Cancer Society’s advocacy arm.
The nonpartisan Congressional Budget Office estimated 18.5 million adults will be subject to the new rules, which will be enforced across 42 states and the District of Columbia. In Indiana, work rules will target about 33% of the state’s Medicaid population. The rules generally wouldn’t apply to children, people 65 or older, or people with disabilities or serious health issues.
Typically, state administrators — not lawmakers — detail how they plan to comply with new federal standards, and they often look to federal regulators for guidance. But officials at the Centers for Medicare & Medicaid Services have yet to tell states how to comply with many aspects of the sweeping budget law, leaving state lawmakers to intervene.
Gov. Mike Braun, a Republican, signed the Indiana bill into law on March 4, making his state the first to set the Medicaid work requirement at three months — the longest period allowed under the federal law.
Republican state Sen. Chris Garten introduced a bill in January, saying it was needed to “align” state law with the new federal Medicaid rules. He also pitched the bill as a way to crack down on “waste, fraud, and abuse” in public programs.
When ineligible people get enrolled, it robs “the truly vulnerable Hoosier who actually needs the help,” Garten said during a January committee hearing.
Democratic state Sen. Fady Qaddoura expressed skepticism during the hearing and questioned the necessity of the legislation. Qaddoura asked Indiana Family and Social Services Administration Secretary Mitch Roob to provide an estimate of the number of ineligible people who enrolled in Medicaid in the state.
“I think very few,” Roob replied. “It’ll never be none.”
After hearing Roob’s answer, Qaddoura said there is no evidence of a widespread problem in Indiana. He accused Republicans of using waste, fraud, and abuse as justification to deny health benefits and food aid to vulnerable Hoosiers.
Garten later called Qaddoura’s accusation a “fundamental mischaracterization” of the bill.
Republicans have said imposing these limits protects the Medicaid program’s longevity.
“We believe in a safety net for our most vulnerable, not a hammock for able-bodied adults that choose not to work,” Garten said. “By tightening these screws, we ensure that our safety net remains sustainable.”
Indiana’s Medicaid enrollment is expected to decrease because of Garten’s legislation, according to an analysis from Indiana’s nonpartisan Legislative Services Agency.
Medicaid helps keep people healthy, so they can continue to work, said Adam Mueller, executive director of the Indiana Justice Project, a nonpartisan legal advocacy organization focusing on health, housing, and food insecurity.
Mueller worries that people will struggle to prove their work history, especially those with nontraditional jobs.
“If the point is to get people engaged, the one month would do it,” Mueller said.
Ultimately, he fears the law will harm Hoosiers with the greatest need for assistance. “They’re going to get tripped up by the bureaucratic hurdles.”
An analysis by the Center on Budget and Policy Priorities predicted that work rules will impose new barriers to coverage and that how states choose to implement the rules will “significantly affect the number of people who lose coverage.” State policy decisions will determine just “how intense the burden is,” the left-leaning think tank found, and opting for a shorter look-back period “will enable more people to enroll.”
Lawmakers in multiple states considered limits. And the same right-leaning lobbying group, the Foundation for Government Accountability, testified in favor of these measures in Arizona, Indiana, and Missouri.
In Missouri, FGA lobbyist James Harris said the measure intends to “move people from dependency and give them back that dignity and pride of work.”
Missouri state Rep. Darin Chappell proposed requiring a three-month look-back period like the measure in Indiana. But the latest version of the bill he sponsored would require applicants to show they were working for only one month before enrolling.
Chappell, a Republican, said his initiative would encourage a “working mindset.”
Anna Meyer, owner of a small bakery in Columbia, Missouri, said the implication is that she and others on Medicaid are lazy. “I have been working since I was 15 years old,” she said. “I’m 43 now.”
Meyer, who voiced her opposition, said she previously had problems submitting information to the state Medicaid agency. She fears new reporting requirements will put her and others at risk of losing coverage, even if they meet the work rule.
She has fibromyalgia, a chronic condition that increases overall sensitivity to pain. She also has food allergies. Medicaid helps pay for medications and doctor visits that keep her healthy and allow her to keep working.
“I work very hard,” Meyer said.
In St. Louis, Jessica Norton, an OB-GYN, treats many Medicaid patients at an Affinia Healthcare clinic. She said they struggle to remain insured even though Missouri extends a full year of Medicaid coverage to eligible women after they give birth. Some of her patients are inexplicably kicked off that coverage by the time of their checkups six weeks after birth. She fears red tape from the new work requirements will make it harder to hang on to insurance, even though pregnant women and new mothers are supposed to be exempt.
Norton criticized lawmakers for the message this policy sends to vulnerable patients. They are saying, “Oh, actually, health care is a privilege, and you have to earn it,” she said.

Nearly two-thirds of adults ages 19 to 64 on Medicaid already work, according to KFF. The reason many of the remaining adults on Medicaid are not working is that they are retired, serving as a caregiver, or too sick, KFF has found.
Some states are not only setting the strictest requirements but also blocking out the optional leniency built into the federal rules.
For example, states may adopt additional exemptions from work rules, such as allowing people to claim a “short-term hardship,” designed to provide continued Medicaid coverage to people with medical conditions that prevent them from working.
Missouri lawmakers are seeking a constitutional amendment to bar their state from offering such optional exemptions. But patient advocates warn these limits would harm the state’s vulnerable residents when they need coverage the most, particularly Missouri’s rural cancer patients.
Often, rural Missouri patients must travel to Kansas City or St. Louis for treatment, disrupting their ability to work, Emily Kalmer, a lobbyist for the American Cancer Society’s advocacy arm, testified at the January hearing. Recognizing this, the federal law provides certain exemptions for this kind of scenario.
But this short-term hardship exemption would be off the table in Missouri.
Time is “very important in the life of a cancer patient or a cancer survivor,” Kalmer said.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.This <a target="_blank" href="https://kffhealthnews.org/insurance/federal-medicaid-work-rules-one-three-months-indiana-missouri/">article</a> first appeared on <a target="_blank" href="https://kffhealthnews.org">KFF Health News</a> and is republished here under a <a target="_blank" href="https://creativecommons.org/licenses/by-nc-nd/4.0/">Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="https://kffhealthnews.org/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="https://kffhealthnews.org/?republication-pixel=true&post=2228139&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>It started building over the summer, fed by news of immigration raids across Southern California, Trump administration plans to share Medicaid data with Immigration and Customs Enforcement, and the passage of state and federal restrictions on immigrant Medicaid eligibility. Then in November, the federal government released a new “public charge” proposal that, if enacted, could block certain immigrants from obtaining permanent legal residency if they or family members have used public benefits, including Medicaid.
Many of González’ clients and their children, often U.S. citizens, still qualify for California’s Medicaid program, known as Medi-Cal, which provides health coverage to over 14 million residents with low incomes or disabilities. But increasingly, they don’t want to enroll or renew their coverage, she said.
“Many people don’t want to apply,” she said. “There are people who say they don’t even want to go outside and water their plants.”
An analysis by KFF Health News found that, from June to December, the latest month for which figures are available, almost 100,000 immigrants without legal status left Medi-Cal, representing about a quarter of all disenrollments in that time frame, even though this group makes up only about 11% of Medi-Cal enrollees.
It marks a reversal in a steady rise in enrollment among immigrants without legal status in California. Until July, sign-ups among this group had risen every month since the state opened Medi-Cal to all low-income residents regardless of immigration status in January 2024.
Tessa Outhyse, a spokesperson for the California Department of Health Care Services, which oversees Medi-Cal, said the enrollment declines can be mostly attributed to the fact that the government restarted eligibility checks that were suspended during the covid-19 pandemic. Indeed, overall Medi-Cal enrollment peaked in May 2023, and has since declined by about 1.6 million.
But two researchers, Leonardo Cuello at Georgetown University’s Center for Children and Families and Susan Babey at the UCLA Center for Health Policy Research, pointed out that California and most other states had fully resumed eligibility checks by mid-2024. In other words, that wouldn’t explain why enrollment has fallen precipitously in the last 12 months or so.
What has changed, Cuello said, is that the federal government passed the One Big Beautiful Bill Act, and executive orders added more changes that are propelling disenrollment.
Surveys Offer Clues
A KFF/New York Times survey found immigrant adults nationally, especially parents, to be increasingly avoiding government programs that help pay for food, housing, or health care, to avoid drawing attention to their or a family member’s immigration status. That included lawfully present residents and naturalized citizens. Parental avoidance of these programs is particularly concerning, Cuello said, because about 1 in 4 children in the U.S. have an immigrant parent, even though most of those children were born in the U.S.
Cuello suspects that may help explain a nationwide enrollment drop of almost 3% in Medicaid and the Children’s Health Insurance Program during the first 10 months of last year, including a 5.6% drop in enrollment among California children, according to data compiled by Georgetown colleagues.
During the first Trump administration, the president broadened public charge criteria to allow consideration of Medicaid use and food and housing assistance. That led many citizen children and other household members to forgo Medicaid and other programs they were eligible for. Some continued to avoid the programs even after several courts blocked implementation and Democratic President Joe Biden rescinded the rule.
“It caused a high level of confusion,” said Louise McCarthy, president and CEO of the Community Clinic Association of Los Angeles County, which represents about 70 health centers in the Los Angeles area. “Community health center staff are still working to undo the effects of the first rule.”
Projected Savings
Currently, only people reliant on cash assistance programs or long-term, government-funded institutionalized care may be considered a public charge risk when applying for a visa to enter the country or to become a legal permanent resident. But under the Trump administration’s proposed rule, Medicaid and other noncash programs could be used to determine whether an immigrant is likely to become dependent on the government. Immigration officers would also have more discretion to label people a public charge.
The Department of Homeland Security’s proposal says the changes are needed because the existing rules hamper the agency’s ability to make decisions about an immigrant’s risk of becoming reliant on government resources. A public comment period for the proposal ended in December.
DHS did not respond to a request about when it plans to make a final decision on the rule. The change would “align with long-standing policy that aliens in the United States should be self-reliant and government benefits should not incentivize immigration,” the proposal states.
The agency projected the change could save federal and state governments almost $9 billion annually from people disenrolling from or forgoing enrollment in public benefit programs.
A KFF analysis of the proposed rule estimated it could result in 1.3 to 4 million people disenrolling from Medicaid or CHIP, including as many as 1.8 million citizen children.
“It’s clearly being weaponized to create fear and anxiety,” said Benyamin Chao, supervising health and public benefits policy manager at the California Immigrant Policy Center. He called the proposal part of an “assault on lawfully present immigrants and U.S. citizens who are family members, and just the general community.”
Public charge fears are expected to decrease enrollment also in anti-hunger programs, such as the Supplemental Nutrition Assistance Program, known in California as CalFresh. Mark Lowry, who heads the Orange County Food Bank, said that that — along with disenrollment related to the One Big Beautiful Bill Act — could overwhelm food pantries, since federal nutrition programs account for the vast majority of food aid.
“There’s no way that the emergency food system has the capacity or resources to address those needs,” he said.
Health Care Needs
Fear of Medi-Cal enrollment doesn’t extend to all immigrants. Juana Zaragoza manages a program in Oxnard that helps mostly Indigenous Mexican farmworkers sign up for Medi-Cal. Overall enrollment and reenrollment has remained steady over the past few months, she said. Neither she nor the community members she serves know much about the public charge proposal, she added.
Often, any concerns they have are outweighed by an immediate need for health care.
“We encounter a lot of people who are balancing: what benefits me now and what benefits me later,” she said. “Some just want to cover their needs in the moment.”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.This <a target="_blank" href="https://kffhealthnews.org/medicaid/public-charge-rule-homeland-security-medicaid-medi-cal-california-immigrants/">article</a> first appeared on <a target="_blank" href="https://kffhealthnews.org">KFF Health News</a> and is republished here under a <a target="_blank" href="https://creativecommons.org/licenses/by-nc-nd/4.0/">Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="https://kffhealthnews.org/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="https://kffhealthnews.org/?republication-pixel=true&post=2178966&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>
KFF Health News chief Washington correspondent Julie Rovner discussed Medicaid cuts on WAMU’s 1A on April 7. She also discussed health care affordability on The Middle With Jeremy Hobson on April 3.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
This <a target="_blank" href="https://kffhealthnews.org/on-air/on-air-april-11-2026-medicaid-cuts-health-care-affordability/">article</a> first appeared on <a target="_blank" href="https://kffhealthnews.org">KFF Health News</a> and is republished here under a <a target="_blank" href="https://creativecommons.org/licenses/by-nc-nd/4.0/">Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="https://kffhealthnews.org/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="https://kffhealthnews.org/?republication-pixel=true&post=2181025&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>
At the Trump administration’s request, a federal judge in Louisiana this week agreed to delay a ruling affecting the continued availability of the abortion drug mifepristone. That angered anti-abortion groups that want the drug, if not banned, at least more strictly controlled. But the administration clearly wants to avoid big abortion fights in the run-up to November’s midterm elections.
Meanwhile, the administration’s proposed budget for fiscal year 2027 calls for more than $15 billion in cuts to programs at the Department of Health and Human Services. It’s a significant number, but less drastic than cuts it proposed for fiscal 2026.
This week’s panelists are Julie Rovner of KFF Health News, Lauren Weber of The Washington Post, Alice Miranda Ollstein of Politico, and Maya Goldman of Axios.
Panelists



Among the takeaways from this week’s episode:
- The Trump administration says it is conducting a thorough scientific review of the abortion pill mifepristone at the Food and Drug Administration. Yet advocates on both sides of the abortion debate think the administration is just trying to buy time to avoid a controversial decision about medication abortion before November’s midterm elections.
- It’s budget time on Capitol Hill. With the unveiling of the president’s spending plan for fiscal 2027, Cabinet secretaries will make their annual tour of congressional committee hearings. HHS Secretary Robert F. Kennedy Jr., whose Hill appearances have been few during his tenure, is scheduled to testify before six separate House and Senate committees before the end of the month.
- Back at HHS, Kennedy appears to be trying to reconstitute the Advisory Committee on Immunization Practices in a way that will enable him to restock it with vaccine skeptics without running afoul of a March court ruling that he violated federal procedures with his replacements last year.
- Continuing his efforts to promote his Make America Healthy Again agenda, Kennedy announced this week that he will launch his own biweekly podcast. He also announced efforts to combat microplastics in the water supply and to get hospitals to stop serving ultraprocessed food to patients.
Plus, for “extra credit,” the panelists suggest health policy stories they read this week that they think you should read, too:
Julie Rovner: The Atlantic’s “HHS Officials’ Year in Purgatory Is Ending,” by Katherine J. Wu.
Maya Goldman: KFF Health News’ “Trump’s Personnel Agency Is Asking for Federal Workers’ Medical Records,” by Amanda Seitz and Maia Rosenfeld.
Lauren Weber: CNN’s “These Common Drug Tests Lead to Tens of Thousands of Wrongful Arrests a Year, Experts Say. One State Is Fighting Back,” by Holly Yan.
Alice Miranda Ollstein: Politico’s “A Slowdown in US Visa Processing Is Wreaking Havoc on Foreign Doctors’ Lives,” by Simon J. Levien.
Also mentioned in this week’s podcast:
- JAMA Internal Medicine’s “Accuracy of Self-Selection for Medication Abortion Using a Prototype Drug Facts Label,” by Lauren J. Ralph, C. Finley Baba, Katherine Ehrenreich, et al.
- KFF Health News’ “Immigrant Seniors Lose Medicare Coverage Despite Paying for It,” by Vanessa G. Sánchez, El Tímpano.
- The New York Times’ “Idaho Cut Services for People With Schizophrenia. Then the Deaths Began,” by Ellen Barry.
- Stateline’s “Medicaid Cuts Could Add Pressure to Already-Stressed Psychiatric Units,” by Nada Hassanein.
- The Washington Post’s “CDC Delays Publishing Report Showing Covid Vaccine Benefits,” by Lena H. Sun.
[Editor’s note: This transcript was generated using both transcription software and a human’s light touch. It has been edited for style and clarity.]
Julie Rovner: Hello, from KFF Health News and WAMU Public Radio in Washington, D.C. Welcome to What the Health? I’m Julie Rovner, chief Washington correspondent for KFF Health News, and I’m joined by some of the best and smartest health reporters covering Washington. We’re taping this week on Thursday, April 9, at 9:30 a.m. As always, news happens fast, and things might have changed by the time you hear this. So here we go.
Today, we are joined via video conference by Lauren Weber of The Washington Post.
Lauren Weber: Hello, hello.
Rovner: Alice Miranda Ollstein of Politico.
Alice Miranda Ollstein: Hi, everybody.
Rovner: And my fellow Michigan Wolverine this national championship week, Maya Goldman of Axios. Go, Blue!
Maya Goldman: Go, Blue.
Rovner: No interview this week, but plenty of news. So let’s get right to it. We’re going to start with reproductive health. On Tuesday, a federal judge in Louisiana ruled for the Trump administration and against anti-abortion forces in a lawsuit over the availability of the abortion pill mifepristone. Wait, what? Please explain, Alice, how the administration and anti-abortion groups ended up on opposite sides of an abortion pill lawsuit.
Ollstein: Yeah. So this has been building for a while, and it is not the only lawsuit of its kind out there. There are several. A bunch of different state attorneys general, who are very conservative and anti-abortion, have been suing the FDA in an attempt to either completely get rid of the availability of the abortion pill mifepristone or reimpose previous restrictions on it. So right now, at least according to federal rules, not according to every state’s rules, you can get it via telehealth. You can get it delivered by mail. You can pick it up at a retail pharmacy. You don’t have to get it in person handed to you from a doctor like you used to. So these lawsuits are attempting to bring back those restrictions or get the kind of national ban that a lot of groups want. And so you have other ones pending: Florida, Texas, Missouri, you have a bunch of ones. So this is the Louisiana version. And the Trump administration, it’s important to note, they are not defending the FDA or the abortion pill on the merits. They are saying, we don’t want this lawsuit and this court to force us to do something. We want to go through our own careful process and do our own internal review of the safety of mifepristone, and then we may decide to impose restrictions. But they’re asking courts to give them the time and space to complete that process and saying, you know, This is our power we should have in the executive branch. And so, in this case, the judge, in ruling for the Trump administration, basically just hit pause. This doesn’t get rid of the case. It just puts a stay on it for now, and that’s important. In some of these other cases, the Trump administration has asked the courts to throw out the case, but that was not the situation here. So this doesn’t mean that abortion pills are going to be available forever. This doesn’t mean nothing’s going to happen, and they’re going to be banned. This just means, you know, we’re kicking the can down the road.
Rovner: I was saying, just to be clear. I mean, we know that this FDA quote-unquote “study” — whether it is or isn’t going on — is part of, kind of, a delaying tactic by the administration, because they don’t want to really make abortion a big front-and-center issue in the midterms. So they’re trying to sort of run the clock out here. Is that not sort of the interpretation that’s going on right now?
Ollstein: That’s what people on both sides assume is going on. It’s really been fascinating how everyone is being kept in the dark about what’s happening inside the FDA — and if this review is even happening, if it’s real, if it’s in good faith, what is it based on? And so it’s become this sort of Rorschach test, where people on the left are saying, you know, They’re laying the groundwork to do a national ban. This is just political cover. They just want to wait until after the midterms, and then they’re going to go for it. And people on the right are saying, you know, The administration is cowardly, and they aren’t really doing anything, and they’re just trying to get us to shut up and be patient. We don’t know if either of those interpretations or neither of them are true.
Rovner: Lauren, you want to add something?
Weber: I just think it’s pretty clear this is also just on a [Health and Human Services Secretary Robert F.] Kennedy [Jr.] priority. I mean, let’s go back. The man … comes from one of the top Democratic political families originally. You know, there’s obviously been a lot of chatter around his anti-abortion beliefs. Now, obviously, he’s on a Republican ticket. I think some of that plays into this as well. And he already has his hand on the stove on so many other hot issues that, [if] I had to guess, I don’t think that they’re trying to rock the boat on this one. … I think, some background context too, to some of what’s going on.
Rovner: We’ll get to some of those hotter issues. But, meanwhile, the Journal of the American Medical Association [Internal Medicine] has a study out this week suggesting that medication abortion is so safe that it could be provided over the counter — that’s without any consultation with a medical professional, either in person or online. This doesn’t feel like it’s going to happen anytime soon, though, right? While we’re still debating the existence of medication abortion in general.
Ollstein: That’s right. I mean, there are a lot of people who can’t get this medication prescribed by a valid doctor right now, let alone over the counter. I will say it is common in a lot of parts of the world to get it over the counter, whereas in the United States, the most common way to have a medication abortion is with a two-pill combination, mifepristone and misoprostol. In a lot of parts of the world, people just use misoprostol alone, and it is effective and it is largely safe. It’s slightly less safe than using both pills together. And so I think there’s a lot of international data out there, and people point to that and advocate for this. And I will say there are activist groups in the United States who are setting up networks, underground networks, to get these pills to people with no doctor’s involvement. And so that is already going on. I think that a lot of people would prefer to get it from a doctor if they could. But because of bans and restrictions, they can’t. And so people are turning to these activist groups.
Rovner: I will point out, as a person who covered the entirety of the fight to have emergency contraception — which is not the abortion pill — made over the counter, it took like, 15 years. It shortened my life covering that story. Lauren, did you want to add something?
Weber: Yeah, I just wanted to say I find it really interesting. Obviously, reproductive issues end up taking 15 years, as you pointed out, to make it over the counter. But there are a lot of things that are considered potentially more dangerous that you can order up in a pretty basic telehealth visit or even just buy in not-so-sketchy ways that the administration is also even looking to deregulate. So I think the differences of access of this compared to other less studied, potentially more unsafe medication is quite striking.
Goldman: Part of [President Donald] Trump’s “Great Healthcare Plan” is making more medications available over the counter. So this is certainly something that they have said they want to do, in general. This is a political nightmare, though, to do that for abortion.
Ollstein: Yeah, and people have been pointing to this and a lot of other policies for a while to argue about something they call abortion exceptionalism, in which people apply a different standard to anything related to abortion, a different safety standard, a different standard of scrutiny than they do to medications for lots of other purposes. And you’ve seen that, and that comes up in lawsuits and political arguments about this. And I think, you know, people can point to this as another example.
Rovner: So last week, we talked about the federal family planning program Title X, which finally got funded after months of delays. But Alice, you warned us that the administration was planning to make some big changes to the program, and now those have finally been announced. Tell us what the plan is for a program that’s provided birth control and other types of primary and preventive care since the early 1970s.
Ollstein: Well, the changes have sort of been announced. They’ve more been teased. What we are still waiting for is an actual rule, like we saw in the first Trump administration, that would impose conditions on the program. And so what we saw recently, it was part of a wonky document called a “Notice of Funding Opportunity,” or NOFO, for those in the D.C. lingo. And basically it was signaling that when groups reapply — they just got this year’s money, but when they reapply for next year’s money — it sets up sort of new priorities and a new focus for the entire program. And what was really striking to me is, you know, this is a family planning program. It was created in the 1970s and it is primarily about delivering contraception to people who can’t afford it around the country, providing it to millions of people who depend on this program, and the word “contraception” did not appear in the entire 70-page document other than an assertion that it is overprescribed and has bad side effects. And instead, they signaled that they want to shift the program to focus on, quote, “family formation.” So this is really striking to me. I think we saw some signs that something like this was coming. You know, about a year ago, there was some Title X money approved to focus on helping people struggling with infertility. But that was sort of just a subset of the program, and now it looks like they want to make that, you know, an overriding focus of the program. So I think when the actual rule to this effect drops, and we don’t know when that will be — will they wait till after the midterms to, you know, avoid blowback? Who knows? I think there will certainly be lawsuits then. But I think right now, this is just sort of a sign of where they want to go in the future. And it’s important to note that it came very quickly on the heels of a big backlash from the anti-abortion movement over the approval of this year’s funding going out to all of the clinics that got it before, including Planned Parenthood clinics. The anti-abortion groups were agitating for Planned Parenthood to be cut off at once, you know, not in the future, right now.
Rovner: Just to remind people that the ban on Planned Parenthood funding from last year was for Medicaid, not for the Title X program.
Ollstein: Right.
Rovner: And that’s why Planned Parenthood got money.
Ollstein: Yes, and Planned Parenthood is not allowed to use any Medicaid or Title X money for abortions, but the anti-abortion groups say it functions like a backdoor subsidy, and so they wanted it to be cut off. So they were very pissed that this money went out to Planned Parenthood. And so very quickly after, the administration put out this document, saying, Look, we are taking things in another direction, and it is not the direction of Planned Parenthood.
Rovner: Lauren, you want to add something?
Weber: Oh, I just wanted to say Alice has really been owning the beat on all the Title X coverage, so …
Rovner: Absolutely.
Weber: … glad we are able to have her explain it to us. But just wanted to throw out a kudos for breaking all the news on that front.
Goldman: Yeah, great coverage.
Rovner: Yes. Very happy to have you for this. Turning to the budget, which is normally the major activity for Congress in the spring, we finally got President Trump’s spending blueprint last week. It does propose cuts to discretionary spending at the Department of Health and Human Services to the tune of about $15 billion, but those cuts are far less deep than those proposed last year. And, as we have noted, Congress didn’t actually cut the HHS budget last year by much at all. And many programs, like the National Institutes of Health, actually got small increases. Is this budget a reflection of the fact that the administration is recognizing that cuts to Health and Human Services programs aren’t actually popular with the public or with Congress, for that matter, going into a midterm election?
Weber: I think it’s that last little piece you mentioned there, Julie. I think it’s the “going into the midterm election.” I think you hit the nail on the head there. Cuts are also not good economically for many Republicans. You know, we saw Katie Britt be one of the — the Alabama Republican senator — be one of the most outspoken senators in general about some of the cuts that were floated for the budget for HHS last year. So I think what you’re hinting at, and what we’re getting at, is that it’s not politically popular, it can be economically problematic, on top of the scientific advances that are not found. So I suspect you are right on that.
Ollstein: The administration knows that this is “hopes and dreams” and will not become reality. It did not become reality last year. It almost never becomes reality. And I think you can see the sort of acknowledgement that this is about sending a message more than actually making policy in things like Title X, because at the same time they put out this guidance from HHS about the future of Title X, moving away from contraception, in the president’s budget he proposed completely getting rid of Title X, completely defunding it, which he has in the past as well. And so why would they put out guidance for a program that doesn’t exist?
Goldman: I think, also, this is the second budget that they’re putting out in this administration, right? So now they are just a little more used to what’s going on, and they have more of their feet under them.
Weber: As a preview for listeners, too, I’m sure we will have Kennedy asked about this budget when he appears in a series of so many hearings next week and the week after. And there were a lot of fireworks last year with him and various members of Congress about the budget. So I am sure that we will hear a lot more on this front in the weeks to come.
Rovner: Yeah, I would say that’s one thing that the budget process does, is when the president finally puts out a budget, the Cabinet secretaries travel to all of the various committees on Capitol Hill to, quote, “defend the president’s budget,” which is sometimes or, I guess in the case of Kennedy, one of the few chances that they get to actually have him in person to ask him questions. But in the meantime, you know, we have the budget, then we have the president himself, who at an Easter lunch last week — that was supposed to be private, but ended up being live-streamed — said, and I quote, “It’s not possible for us to take care of day care, Medicare, Medicaid, all these individual things.” The president went on to say that states should take over all that social spending, and the only thing the federal government should fund is, quote, “military protection.” Did I just hear a thousand Democratic campaign ads bloom?
Goldman: I think this is a prime example of when you should take Trump seriously, but not literally. I don’t think that there’s any world, at least in the foreseeable future, where the federal government isn’t funding Medicare. But, you know, you certainly have to watch at the margins. It’s like, it’s not a secret that this is something that they’re interested in cutting back spending on. It’s super politically difficult to do that, and they know that, and that’s part of why, which I’m sure we’ll talk about in a little bit, they bumped up the payment rate for 2027 to Medicare Advantage plans.
Rovner: Which we will get to.
Goldman: Yeah, so I mean, it’s certainly an eye-opening statement, and you should remember it. But I don’t think that we’re in immediate jeopardy here.
Rovner: This is the president who ran in 2024, you know, saying that he was going to protect Medicare and Medicaid. I mean, it’s been, you know, against some of the recommendations of his own administration. I was just sort of shocked to see these words come out of his mouth. Lauren, you wanted to say something?
Weber: I mean, it’s not that surprising, though. I mean, look at what the One Big Beautiful Bill [Act] did to Medicaid. He’s already pushed through massive Medicaid cuts, which are essentially being offloaded to the states. So, I mean, I think this ideology has already borne out and will continue to bear out, and obviously it’s happening amid the backdrop of a war. So that plays into, obviously, the commentary as well.
Rovner: Well, meanwhile, Republicans are still talking about doing another budget reconciliation bill, the 2.0 version of last year’s Big Beautiful Bill, except this time it’s essentially just to fund the military and ICE [Immigration and Customs Enforcement] and border control, because Democrats won’t vote for those things, at least they won’t vote for additional military spending. What are the prospects for that to actually happen? And would Republicans really be able to do it if those programs are paid for with more cuts to Medicare and/or Medicaid, as some have suggested?
Goldman: You know, my co-worker Peter Sullivan wrote about this last week, and there was a lot of blowback from politicos, from advocates, from, you know, kind of across the spectrum of groups there. I think that it would be extremely politically unpopular, especially going into the midterms, to use health care as an offset. But I would say that Republicans are pretty good at rhetoric, right? That’s one of the things that they’re known for right now, and there’s always a way to spin it.
Rovner: Alice and I spoke to a group earlier this week, and I went out on a limb and predicted that I didn’t think Republicans could get the votes for another big budget reconciliation this year. I mean, look at how close it was last year. The idea of cutting any deeper seems to me unlikely, just given the margins that they have.
Goldman: And I think that is something that you do in between election years. That’s not something you do in an election year.
Rovner: That’s true, yes … you do tend to see these bigger bills in the odd-numbered years rather than the even-numbered years, but …
Ollstein: And I think it’s important to remember that the reason Republicans are in this bind and that they feel like they have to keep reconciliation nearly focused on funding immigration enforcement is because Democrats refuse to fund immigration enforcement. And so they feel pressured to put all their effort and political capital towards that, and don’t want to mess that up by adding a bunch of other health care things that could cause fights and lose them votes.
Goldman: The money has got to come from somewhere.
Rovner: And health care is where all the money is. Speaking of Medicare and Medicaid, where most of the money is, there is news on those fronts, too. Maya, as you hinted on Medicare, the administration is out with its payment rule for private Medicare Advantage plans for next year. And remember, we talked about how HHS was going to really go after overbilling in Medicare Advantage and cut reimbursement dramatically? Well, you can forget all that. The final rule will provide plans with a 2.48% pay bump next year. That’s compared to the less than 1% increase in the proposed rule. That’s a difference of about $13 billion. The final rule also eliminated many of the safeguards that were intended to prevent overbilling. What happened to the crackdown on Medicare Advantage? Are their lobbyists really that good?
Goldman: Their lobbyists are pretty good. This was a year where there were — I think CMS [the Centers for Medicare & Medicaid Services] said there were a record number of public comments on their proposed rate, flat rate increase, flat rate update. But I think it’s also not that surprising. Historically, the final rate announcement for Medicare Advantage is almost always a little higher than the proposed because they incorporate additional data from the end of the previous year that wasn’t available when first rate is proposed, the initial rate is proposed. But certainly they backed away from a big change to risk adjustment, or, like, the way to adjust payment based on how sick a plan’s enrollees are. You get more pay …
Rovner: Because that’s where the overbilling was happening, that we’d seen a lot of these wonderful stories that plans were basically, you know, inventing diagnoses for patients who didn’t necessarily have them or didn’t have a severe illness, and using that to get additional payments.
Goldman: Right. And they did move forward with a plan to prevent diagnoses that are not linked to information that’s in a patient’s medical chart from being used for risk adjustment. But a lot of plans had said, like, Yeah, this is, that’s the right thing to do, and it’s not going to be that impactful for us. You know, overall, this is a win for health insurance. I think one thing to note is that Chris Klomp, the director of Medicare, said, We’re still really focused on trying to right-size this program. That’s still a priority for us as an administration, but we also want to safeguard it. And so I think insurers are not off the hook entirely. There’s still going to be a lot of scrutiny, but their lobbyists are pretty good. And you know, no one wants to be seen as the candidate that cuts Medicare.
Rovner: And we have seen this before, that when Congress cuts “overfunding” for Medicare Advantage, the plans, seeing that they can’t make its big profits, drop out or they cut back on those extra benefits. And the beneficiaries complain because they’re losing their plans, or they’re losing their extra benefits, and they don’t really want to do that in an election year either, because there are a lot of people, many millions of people, who vote who are on these plans. So, in some ways, the plans have the administration over a political barrel, in addition to how good their lobbyists are.
Well, apparently, one group that HHS is still cracking down on are legal immigrants with Medicare. Most of the publicity around the health cuts in last year’s budget bill focused on the cuts to Medicaid. But we at KFF Health News have a story this week about legal immigrants who’ve paid into the Medicare system with their payroll taxes for years and are now being cut off from their Medicare coverage. This is apparently the first time an entire category of beneficiaries are having their Medicare taken away. I’m surprised there hasn’t been more attention to this, or if it’s just too much all happening at once.
Ollstein: I mean, there’s a lot happening at once, and even just in the space of immigrants’ access to health care, there is so much happening at once. And so this is obviously having a huge impact on a lot of people, but so are 100 other things. And I think, you know, the zone has been flooded as promised. And really, state officials who are also dealing with a thousand other things, Medicaid cuts, you know, these federal changes, work requirements, are grappling with this as well.
Rovner: Lauren, you wanted to add something?
Weber: Yeah. I mean, I thought it was, there was a striking quote in the story from Michael Cannon, who basically said, The reason this isn’t resonating is because this won’t upset the Republican base. And I think that’s a striking quote to be considered.
Rovner: Michael Cannon, libertarian health policy expert, just kind of an observer to this one. But yeah, I think that’s true. I mean, or at least the perception is that these are not Republican voters, although, you know, as we’ve seen, you know, Congress has tried to take aim at people they think aren’t their voters, and it’s turned out that those are their voters. So we will see how this all plays out.
Well, at the same time that this is all going on, the folks over at the newsletter “Healthcare Dive” are reporting that the Centers for Medicare & Medicaid Services are trying to embark on all these new initiatives on fraud, and work requirements, and artificial intelligence with a diminished workforce. While CMS lost far fewer workers in the DOGE [Department of Government Efficiency] cuts last year than many other of the HHS agencies — it was in the hundreds rather than the thousands — CMS has long been understaffed, given the fact that it manages programs that provide health insurance to more than 160 million Americans through not just Medicare and Medicaid, but also the Children’s Health Insurance Program and the Affordable Care Act. I know last week, FDA Commissioner Marty Makary said he wants to hire more workers to replace the 3,000 who were RIF’ed or took early retirement there at the FDA. And CMS does have lots of job openings being advertised. But it’s hard to see how replacing trained and experienced workers with untrained, inexperienced ones are going to improve efficiency, right?
Goldman: Tangentially, I was talking to a health insurance executive yesterday who was saying that his team is so much bigger than CMS, and they cover a fraction of the market, and they’re often the ones coming to CMS and proposing ideas and working with CMS on it. I don’t, I think that is a dynamic that far predates this administration, but …
Rovner: Oh, absolutely.
Goldman: But it’s certainly interesting. And … CMS has very ambitious plans, and not that many people to carry them out. But, you know, I think one thing that I also want to note is that when I talk to trade associations and stakeholders about this CMS, they are generally like, pretty support- … like, they say that they think they’re being heard, and they think that CMS and the career staff are doing, you know, the same kind of caliber of work that they’ve been doing, which I think is notable.
Rovner: And as we have mentioned many times, you know, Dr. [Mehmet] Oz, the head of CMS, is very serious about his job and doing a lot of really interesting things. It’s just, it’s hard, you know, in the federal government, if you don’t have the resources that you want to … if you don’t have the resources to match your ambitions. Let’s put it that way.
Well, meanwhile, on the Medicaid front, we’re already seeing states cutting back, and some of the results of those cutbacks. Stateline has a piece on how psychiatric units are at risk of being shut down due to the Medicaid cuts, since they often serve a disproportionate number of low-income people and also tend to lose money. And The New York Times has a heartbreaking story of an Idaho Medicaid cutback of a program that had provided home visits to people living in the community with severe mental illness, until those people who lost the services began to die or to end up back in more expensive institutional care. Now the state has resumed funding the program, but obviously will end up having to cut someplace else instead. I know when Republicans in Congress passed the cuts last year, they said that people on Medicaid who were not the able-bodied working-age populations wouldn’t see their services cut. But that’s not how this is playing out, right?
Weber: I just think the story by Ellen Barry, who you should always read on mental health issues in The New York Times, “Idaho Cut Services for People With Schizophrenia, Then the Deaths Began,” is such an illustrative example of unintended consequences from these cuts. And the reason that they’re being reversed — by Republican legislators, no less — in Idaho, is because it’s more expensive to have cut the money from it than it is efficient. I mean, what they found was, is that after they cut the money to the schizophrenia program, they saw this massive uptick in law enforcement cases and hospitalizations, uninsured hospitalizations, that this avoided. And I think it’s a real canary in the coal mine situation, because we’re only starting to see these states cut these things off. And this was a pretty immediate multiple-death consequence. And I think we’re going to see a lot of stories like this, of a variety of programs that we all don’t even have any idea that exist in the safety net across the country that are being chipped away at.
Rovner: Well, turning to other news from the Department of Health and Human Services, we’re getting some more competition here at What the Health? Health secretary Kennedy has announced he’ll be unveiling his own podcast, called The Secretary Kennedy Podcast, next week. He promises to, according to the trailer posted online on Wednesday, quote, “name the names of the forces that obstruct the paths to public health.” OK then, we look forward to listening.
Meanwhile, in actual secretarial work, the secretary this week also unveiled changes to the charter of the Advisory Committee on [Immunization] Practices after a federal judge last month invalidated both the replacement members that he’d appointed last year and the changes made to the federally recommended vaccine schedule. So what’s going to happen here now? Will this get around the judge’s ruling by watering down the expertise that members of this advisory committee are supposed to have in vaccines? And why hasn’t the administration appealed the judge’s ruling yet?
Goldman: You know, I don’t have actual answers to this, but I do wonder and speculate that this is going to end up being some kind of legal whack-a-mole situation where the secretary and HHS says, OK, you don’t like it that way? We’ll do it this way, and then they’ll do it another way, and advocates will sue, and we’ll see how this plays out going forward in the courts. I think this is not the end of the story. Even though the judge’s decision was a big win for vaccine advocates, it’s just we’re in the midpoint, if that.
Rovner: And Lauren, speaking of vaccines, your colleague Lena H. Sun has quite the scoop on HHS and vaccine policy.
Weber: Yeah, Lena Sun is always delivering. She found out that the acting director of the CDC [Centers for Disease Control and Prevention] at the time delayed publication of a report showing that the covid-19 vaccine[s] cut the likelihood of emergency department visits and hospitalizations for healthy adults last winter by about half. So even though Kennedy is not talking more about vaccines, it appears that, based on this reporting, that some of his underlings are not necessarily touting the benefits of vaccine, so to speak. And I’m very curious, going back to Kennedy’s podcast, I found the rollout of that so interesting because the teaser was very leaning into the Kennedy that got elected, you know, someone who speaks about, you know, dark truths that are hidden from the public, and so on. And then the press team had these statements of, like, Kennedy will investigate the affordability of health costs and food and nutrition. And I think this dichotomy of who Kennedy is and who the White House and the press secretary and HHS want Kennedy to be before the midterms really could come to a head in this podcast. So I think we will all be listening to hear how that goes.
Rovner: Yeah, we keep hearing about how the secretary is being, you know, sort of put on a leash, if you will. And, you know, told to downplay some of his anti-vaccine views and things like this. And that seems quite at odds with him having his own podcast. Alice, do you want to …?
Weber: I guess, it depends on who’s editing the podcast and who they have on. I’m just very … you could even tell from the trailer to how his press secretary presented it, there was an interesting differential in framing, and I am curious how that plays out as we see guests on it.
Ollstein: I mean, it’s also worth noting that this is an administration of podcasters. I mean, you have Kash Patel, you have so many of these folks who have a history of podcasting, clearly have a passion for it, just can’t let it go while working a full-time, high-pressure government job.
Rovner: We shall see. Meanwhile, HHS, together with the Environmental Protection Agency, is waging war on microplastics, those nearly too impossible to detect bits of plastic that are getting into our lungs and stomachs and body tissues through air and water and food. The plan here seems to be to find ways to detect exactly how much microplastics we are all getting in our water and what the health impacts might be, since we don’t have enough information to regulate them yet. I would think this would be one of those things that pleases both MAHA [Make America Healthy Again] and the science community, right? Or is it just, as one MAHA supporter called it, theater?
Goldman: I think this is a great example of the, you know, part of the reason why MAHA is so interesting to such a wide swath of people. Like, there’s a lot of legitimate concern, not that other concerns aren’t necessarily legitimate, but there’s a lot of concern over, from the scientific community, over microplastics. I’m honestly surprised that we’re this far into the administration with this announcement. I would have thought that this is something they would have done sooner, but they obviously had other priorities as well.
Rovner: Well. Finally, this week, speaking of other priorities, HHS Secretary Kennedy and CMS Administrator Dr. Oz are declaring war on junk food in hospitals. Again, this seems like a popular and fairly harmless crusade; hospitals shouldn’t be serving their patients ultraprocessed food. Except, almost as soon as the announcement came out, I saw tons of pushback online from doctors and nurses who worried about patients for whom sugary food or drinks are actually medically indicated, or who, because of medications they’re taking, or illnesses they have, can only eat, or will only eat, highly palatable, often processed food. Nothing in health care is as simple as it seems, right?
Weber: I think what’s also interesting is one of my favorite examples in the memo they put out was they hope that every hospital, as an example, could serve quinoa and salmon. And I just am curious to see how fast that gets implemented. And it’s a very valid — a lot of people complain about hospital food. It’s a very valid thing to push for better food. But I also question, as I understand it, this seems more like a carrot than a stick when it comes to the regulation they put out.
Rovner: As it were.
Weber: As it were. And so I’m curious to see how it gets implemented. That said, there are hospitals that have taken it upon themselves — the Northwell [Health] example in New York is a good example — to really improve their hospital food. And frankly, it’s a money maker. If your food’s better, people come to your hospital, especially in an urban area where there is hospital competition. So you know, like most MAHA topics, there’s a lot of interesting points in there, and then there’s a lot of what’s the reality and what’ actually going to happen. And so I’ very curious to see how this continues to play.
Rovner: I did a big story, like, 10 years ago on a hospital chain that had its own gardens, that literally grew its own healthy food. So this is not completely new but, again, interesting.
All right, that is this week’s news. Now it’s time for our extra-credit segment. That’s where we each recognize a story we read this week we think you should read, too. Don’t worry if you miss it. We will post the links in our show notes on your phone or other mobile device. Alice, why don’t you start us off this week?
Ollstein: I have a piece from my co-worker Simon [J.] Levien, and it is called “A Slowdown in US Visa Processing Is Wreaking Havoc on Foreign Doctors’ Lives.” This is about thousands of doctors around the country who are from other countries that are placed on, you know, a list by the Trump administration of places where they want to scrutinize and limit the number of immigrants coming from there. And so these are people who are already here, already practicing, have poured years into their training, have been living here, and, in some cases, are the only folks willing to work in certain areas that have a lot of medical shortages, and they just can’t practice because their paperwork isn’t getting processed in time. And so they’re sort of in this scary limbo, and that’s putting these hospitals and clinics that they work in in a really tough bind. And so they’re hammering the Trump administration to give them answers about what their fate is. You know, they’re not trying to deport them yet, but they’re not allowing them to continue working either.
Rovner: For an administration that’s been pushing really hard to improve rural health care, this does not seem to be a way to improve rural health care. Maya.
Goldman: My extra credit this week is called “Trump’s Personnel Agency Is Asking for Federal Workers’ Medical Records.” It’s a great KFF Health News scoop from Amanda Seitz and Maia Rosenfeld. It’s a really great example of the administration, you know, sort of moving in silence, doing these small regulatory announcements that could have big impact. Basically, the Office of Personnel Management is asking for personally identifiable medical information from health insurers, and its reasoning is to analyze costs and improve the health system, but they could get very detailed medical information from federal employees, including things like, did they get an abortion? Are they undergoing gender-affirming care? And, obviously, there is a strong concern that that could be used against them.
Rovner: Yeah … this was quite a scoop. Really, really interesting story. Lauren.
Weber: Mine was a pretty alarming story by Holly Yan at CNN: “These Common Drug Tests Lead to Tens of Thousands of Wrongful Arrests a Year, Experts Say. One State Is Fighting Back.” And basically there’s this type of drug test that the scientists have found is not that effective, and it’s led to things like bird poop being scraped off a man’s car appearing on a drug test as cocaine, a great-grandmother’s medication testing positive for cocaine, and a toddler’s ashes registering as meth or ecstasy, and horrible legal and other consequences of this kind of misdiagnosis in the field. And the reason these drug tests are often done is because they’re cheaper. There’s a more expensive, more accurate version, but these are cheaper. They’re done in the field. But the potential side effects and horrible, wrongly accused effects are quite large, and so Colorado has passed this law to try and move away from this. And it’s curious to see if other states will follow suit.
Rovner: Yeah, this was something I knew nothing about until I read this story. My extra credit this week is from The Atlantic by Katherine [J.] Wu, and it’s called “HHS Officials’ Year in Purgatory Is Ending.” And it’s about how some of the very top career officials from the NIH [National Institutes of Health], the CDC, and other agencies have, after having been put on leave more than a year ago, finally been reassigned to far-flung outposts of the Indian Health Service in the western United States. They got news of their proposed reassignments with little description of their new roles and only a couple of weeks to decide whether to move across the country or face termination. Now, if these officials’ skills matched those needed by the Indian Health Service, this all might make some sense. But what the IHS most needs are active clinicians: doctors and nurses and social workers and lab technicians. And those who are now being reassigned are largely managers, including — and here I’m reading from the story, quote — “the directors of several NIH institutes, leaders of several CDC centers, a top-ranking official from the FDA tobacco-products center, a bioethicist, a human-resources manager, a communications director, and a technology-information officer.” The Native populations who are ostensibly being helped here aren’t very happy about this, either. Former Biden administration Interior Secretary Deb Haaland, a Native American who’s now running for governor in New Mexico, called the reassignment proposals, quote, “shameful” and “disrespectful.” Also, and this is my addition, not a very efficient use of human capital.
OK, that’s this week’s show. Thanks this week to our fill-in editor, Mary-Ellen Deily, and our producer-engineer, Francis Ying. A reminder: What the Health? is now available on WAMU platforms, the NPR app, and wherever you get your podcasts — as well as, of course, kffhealthnews.org. Also, as always, you can email us your comments or questions. We’re at whatthehealth@kff.org. Or you can find me on X @jrovner, or on Bluesky @julierovner. Where do you guys hang these days? Maya.
Goldman: I am on LinkedIn under my first and last name, Maya Goldman, and on X at @mayagoldman_.
Rovner: Alice.
Ollstein: I’m on Bluesky @alicemiranda and on X @AliceOllstein.
Rovner: Lauren.
Weber: Still @LaurenWeberHP on both X and Bluesky.
Rovner: We will be back in your feed next week. Until then, be healthy.
Credits
Click here to find all our podcasts.
And subscribe to “What the Health? From KFF Health News” on Apple Podcasts, Spotify, the NPR app, YouTube, Pocket Casts, or wherever you listen to podcasts.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.This <a target="_blank" href="https://kffhealthnews.org/podcast/what-the-health-441-mifepristone-trump-budget-request-hhs-april-9-2026/">article</a> first appeared on <a target="_blank" href="https://kffhealthnews.org">KFF Health News</a> and is republished here under a <a target="_blank" href="https://creativecommons.org/licenses/by-nc-nd/4.0/">Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="https://kffhealthnews.org/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="https://kffhealthnews.org/?republication-pixel=true&post=2181013&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>“The first time, it’ll ring interminably. Next time, it’ll go to a voicemail that just hangs up on you,” said the 48-year-old, who lives in Delaware. “Sometimes you’ll get a person who says they’re not the right one. They transfer you, and it hangs up. Sometimes, it picks up and there’s just nobody on the line.”
She spent months trying to figure out whether her Medicaid coverage had been renewed. As of late March, she hadn’t been reapproved for the year for the state-federal program, which provides health insurance for people with low incomes and disabilities.
Crouch, who suffered a debilitating brain aneurysm a decade ago, also has Medicare, which covers people who are 65 or older or have disabilities. Medicaid had been paying her monthly Medicare deductibles of $200, but she’d been on the hook for them for the past three months, straining her family’s fixed income, she said.
Crouch’s challenges with Delaware’s Medicaid call center aren’t unique. State Medicaid agencies can struggle to keep enough staff to help people sign up for benefits and field calls from enrollees with questions. A shortage of such workers can keep people from fully using their benefits, health policy researchers said.
Now, congressional Republicans’ One Big Beautiful Bill Act, which President Donald Trump signed into law last summer, will soon demand more from staff at state agencies in places where lawmakers expanded Medicaid to more low-income adults — nearly all states and the District of Columbia.
Under the law, which is expected to reduce Medicaid spending by almost $1 trillion over the next eight years, these staffers will have to not only determine whether millions of enrollees meet the program’s new work requirements but also verify more frequently that they qualify for the program — every six months instead of yearly.
KFF Health News reached out to agencies that will need to stand up the work rules, and many said they’ll need additional staff.
The mandates will put extra strain on an already-stressed workforce, potentially making it harder for enrollees like Crouch to get basic customer service. And many could lose access to benefits they’re legally entitled to, said consumer advocates and health policy researchers, some of them with direct experience working at state agencies.
States are already “struggling significantly,” said Jennifer Wagner, the director of Medicaid eligibility and enrollment at the Center on Budget and Policy Priorities and a former associate director of the Illinois Department of Human Services. “There will be significant additional challenges caused by these changes.”
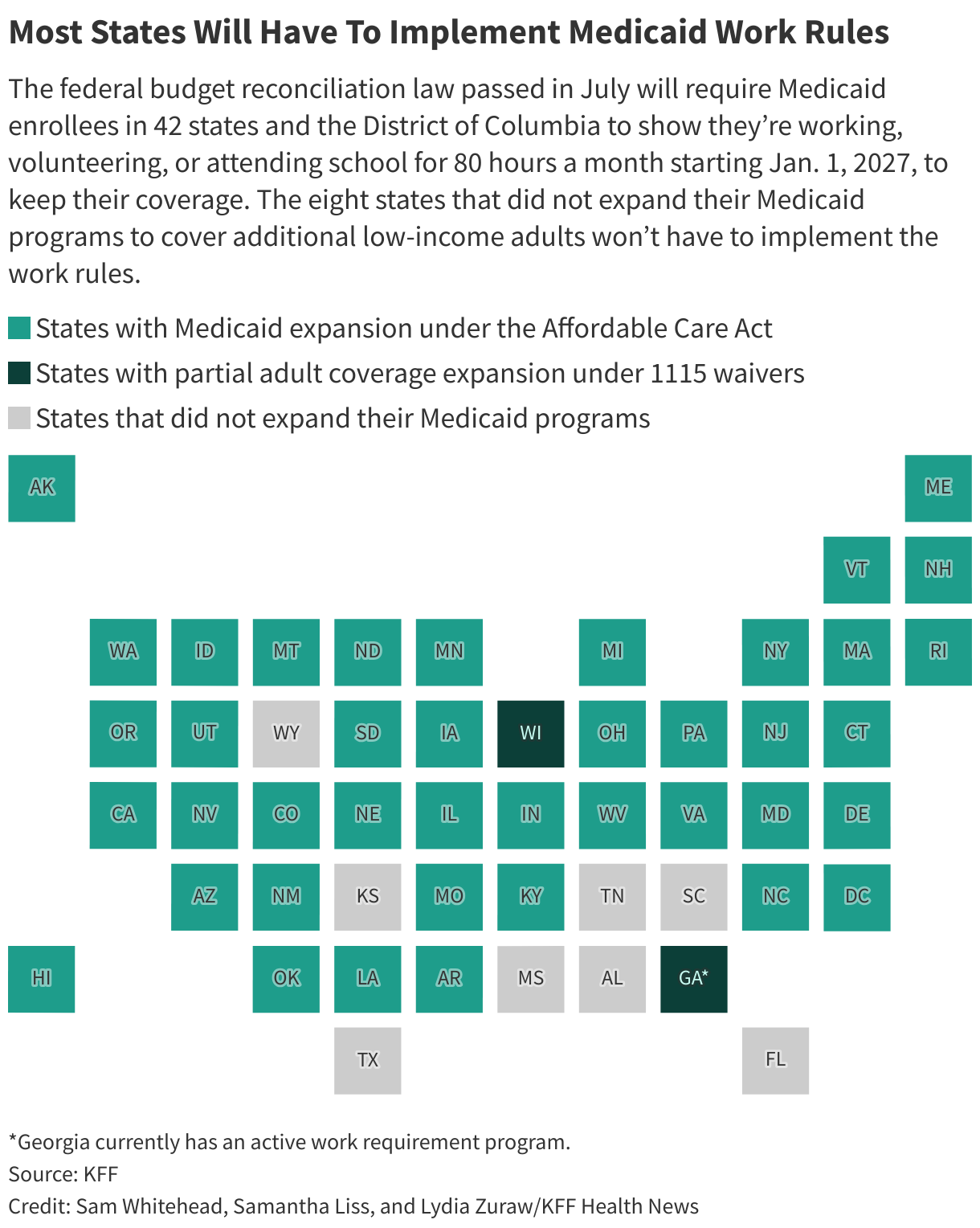
Long Wait Times for Help
Republicans argue the Medicaid changes, which will take effect Jan. 1, 2027, in most states, will encourage enrollees to find jobs. Research on other Medicaid work requirement programs has found little evidence they increase employment.
The Congressional Budget Office estimated the rules would cause more people to lose health coverage by 2034 than any other part of the GOP budget law. It said last year more than 5 million people could be affected.
Many states don’t have the staff to process Medicaid applications or renewals quickly, said consumer advocates and researchers.
The Centers for Medicare & Medicaid Services tracks whether states can handle the most common type of benefit application within a 45-day window.
In December, about 30% of all Medicaid and Children’s Health Insurance Program, or CHIP, applications in Washington, D.C., and Georgia took more than 45 days to process. More than a quarter took that long in Wyoming. In Maine, 1 in 5 applications missed that deadline.
CMS began publicly sharing state Medicaid call center data in 2023, revealing a taxed system, researchers and consumer advocates said.
In Hawaii, people waited on the phone for more than three hours in December. They waited for nearly an hour in Oklahoma, and more than an hour in Nevada.
In 2023, state Medicaid agencies began making sure enrollees who were protected from being dropped from the program during the covid pandemic still qualified for coverage. That Medicaid unwinding process didn’t go well in many states, and more than 25 million lost their benefits.
Health policy researchers and consumer advocates say rolling out the new Medicaid rules will be a bigger challenge. The Medicaid work rules will require extensive IT system changes and training for workers verifying eligibility on a tight timeline.
“It is a much larger scale of administrative complexity,” said Sophia Tripoli, senior director of policy at Families USA, a health care consumer advocacy organization.
After months of trying to get someone on the phone, Crouch said, she finally got answers to questions about her Medicaid benefits after writing to the office of U.S. Rep. Sarah McBride (D-Del.). McBride’s office contacted the state’s Medicaid agency, which eventually called with an update, Crouch said.
Crouch didn’t qualify for Medicaid after all. She said that had never come up in two years of interactions with the state.
“It makes absolutely no sense” that the state never realized she shouldn’t have been on the program, Crouch said.
Delaware’s Medicaid agency didn’t respond to requests for comment on Crouch’s situation.
States Short-Staffed for Medicaid
Some states told KFF Health News in late March that they’ll need more staff to roll out the work rules effectively.
Idaho said it has 40 eligibility worker vacancies. New York estimated it will need 80 new employees to handle the additional administrative work, at a cost of $6.2 million. Pennsylvania said it has nearly 400 open positions in county human services offices in the state. Indiana’s Medicaid agency has 94 open positions. Maine wants to hire 90 additional staffers, and Massachusetts wants to hire 70 more.
As of early March, Montana had filled 39 of 59 positions state officials projected it would need. The state still plans to roll out the rules early, starting July 1, despite its long struggle with system backlogs that applicants said have delayed benefits.
Missouri’s social services agency has been cutting staff and has 1,000 fewer front-line workers than it did roughly a decade ago — with more than double the number of enrollees in Medicaid and the Supplemental Nutrition Assistance Program, or SNAP, according to comments Jessica Bax, the agency director, made during a public meeting in November.
“The department thought that there would be a gain in efficiency due to eligibility system upgrades,” Bax said. “Many of those did not come to fruition.”
States could have a hard time finding people interested in taking those jobs, which require months-long training, can be emotionally challenging, and generally offer low pay, said Tricia Brooks, a researcher at the Georgetown University Center for Children and Families.
“They get yelled at a lot,” said Brooks, who formerly ran New Hampshire’s Medicaid and CHIP customer service program. “People are frustrated. They’re crying. They’re concerned. They’re losing access to health care, and so sometimes it’s not an easy job to take if it’s hard to help someone.”
States are paying government contractors millions of dollars to help them comply with the new federal law.
Maximus, a government services contractor, provides eligibility support, such as running call centers, in 17 states that expanded Medicaid and interacts with nearly 3 in 5 people enrolled in the program nationally, according to the company.
During a February earnings call, company leadership said Maximus can charge based on the number of transactions it completes for enrollees, independent of how many people are enrolled in a state’s Medicaid program.
Maximus has “no one-size-fits-all approach” to the services it offers or the way it charges for those services, spokesperson Marci Goldstein told KFF Health News.
The company, which reported bringing in $1.76 billion in 2025 from the part of its business that includes Medicaid work, expects that revenue to continue to grow, even as people fall off the Medicaid rolls, “because of the additional transactions that will need to take place,” David Mutryn, Maximus’ chief financial officer and treasurer, said during the earnings call.
Losing Medicaid health coverage isn’t just an inconvenience, since many people enrolled in the program probably don’t make enough money to pay for health care on their own and may not qualify for financial help for Affordable Care Act coverage, said Elizabeth Edwards, a senior attorney with the National Health Law Program.
People could be unable to afford medications or get essential care, which could lead to “devastating” health impacts, she said.
“The human stakes of this are people’s lives,” she said.
KFF Health News correspondents Katheryn Houghton and Samantha Liss contributed to this report.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.This <a target="_blank" href="https://kffhealthnews.org/medicaid/medicaid-cuts-work-requirements-state-staff-shortages/">article</a> first appeared on <a target="_blank" href="https://kffhealthnews.org">KFF Health News</a> and is republished here under a <a target="_blank" href="https://creativecommons.org/licenses/by-nc-nd/4.0/">Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="https://kffhealthnews.org/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="https://kffhealthnews.org/?republication-pixel=true&post=2178951&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>MARQUETTE, Mich. — Providing abortions was the last thing Shawn Brown thought she’d be doing when she opened an urgent care clinic in this remote town in Michigan’s Upper Peninsula.
But she also wasn’t expecting the Planned Parenthood in Marquette to shut down last spring. Roughly 1,100 patients relied on that clinic each year for cancer screenings, IUD insertions, and medication abortions. Now the area has no other in-person resource for abortions. “It’s a 500-mile stretch of no access,” Brown said.
So the doctor, who describes herself as “individually pro-life,” added medication abortions to Marquette Medical Urgent Care’s already busy practice, which treats a steady flow of kids with the flu, college students with migraines, and tourists with skiing injuries.
At least 38 abortion clinics shut down last year in states where they’re still legal, according to data collected by I Need an A, a project supported by a number of nonprofits that helps people find abortion options. Even states that recently passed constitutional amendments protecting abortion rights, such as Michigan, have had clinics close since the U.S. Supreme Court overturned Roe v. Wade in 2022. And as rural hospitals shutter labor and delivery units, patients are losing access to pregnancy care. “You cannot have a high-risk pregnancy up here,” Brown said. “It’s a scary place.”
Now communities are coming up with alternatives, such as Brown’s urgent care.
The idea that urgent cares “could be an untapped solution to closures for abortion clinics across the country is really exciting,” said Kimi Chernoby, the chief operating and legal officer at FemInEM, a national nonprofit that works to improve professional training and patient outcomes for women in emergency medicine.
One patient at the Marquette urgent care on a recent day was a woman whom KFF Health News agreed to identify by only her first initial, “A,” to protect her medical privacy. She drove more than an hour on snowy backroads while her kids were in day care to get to her appointment.
Her youngest is still a baby, A said, and she got pregnant again while taking the progestin-only birth control pill, which is less likely to interfere with breast milk production but slightly less effective than the regular pill.
“Financials, housing, vehicles — it’s a lot,” she said. And another baby is “just not something that we could really do even at this time.”
She said she was making the long round trip because receiving abortion care in an office felt more secure than being treated by “someone that I’ve never met, or receiving meds that were just shipped to me.”

Face-to-Face Care
In one of the urgent care’s exam rooms, A sat in a chair against the wall, waiting quietly for the doctor. Viktoria Koskenoja, an emergency medicine physician, knocked on the door and then greeted her warmly, pulling up a stool across from her.
“Are you confident in your decision that you want to go ahead? Or do you want to talk about options?” she said.
“No, I’m pretty set on it,” A said.
Koskenoja previously worked at Planned Parenthood. When she learned its Marquette clinic was closing, she started crying and making calls. She recalled asking everyone she knew in health care in Marquette: “What are we going to do?”
One of her first calls was to Brown, a friend and fellow emergency medicine doctor. Their families harvest maple syrup together each spring.
In the wake of the Planned Parenthood closure, Koskenoja convened a community meeting downtown at the Women’s Federated Clubhouse, an 1880s-era building where guests sip from gold-rimmed china teacups on lace tablecloths. The goal: brainstorm new ways to provide abortion access in the Upper Peninsula.
Planned Parenthood of Michigan officials said that growing financial challenges and the Trump administration’s cuts to funding, including for the public insurance program Medicaid, had prompted the closures of some brick-and-mortar clinics in the state.
Plus, the availability of pills by mail exploded after the 2022 Dobbs v. Jackson Women’s Health Organization decision overturned Roe. As abortion became illegal in many states, telehealth abortions went from 5% of all abortions provided to 25% by the end of 2024, according to #WeCount, a national reporting project that tracks shifts in abortion volume.
Planned Parenthood of Michigan’s telehealth appointments increased 13% for patients in the Upper Peninsula after the Marquette location closed, said Paula Thornton Greear, president and CEO of Planned Parenthood in the state.
All the abortion patients Koskenoja sees at the urgent care have one thing in common: They want to talk to someone in person.
“I had a patient order the pills online and then get scared to use them because they felt like they were going to screw it up, or they weren’t sure they could rely on the pills,” she said. “So they literally came in here with the pills in their hand.”
Others have medical complications or need an ultrasound to determine how far along they are with the pregnancy.
“It annoys me that telehealth is considered an acceptable thing in rural areas,” Koskenoja said. “As though we’re not the human beings that like talking to human beings and looking someone in the eye, especially when something serious is going on.”

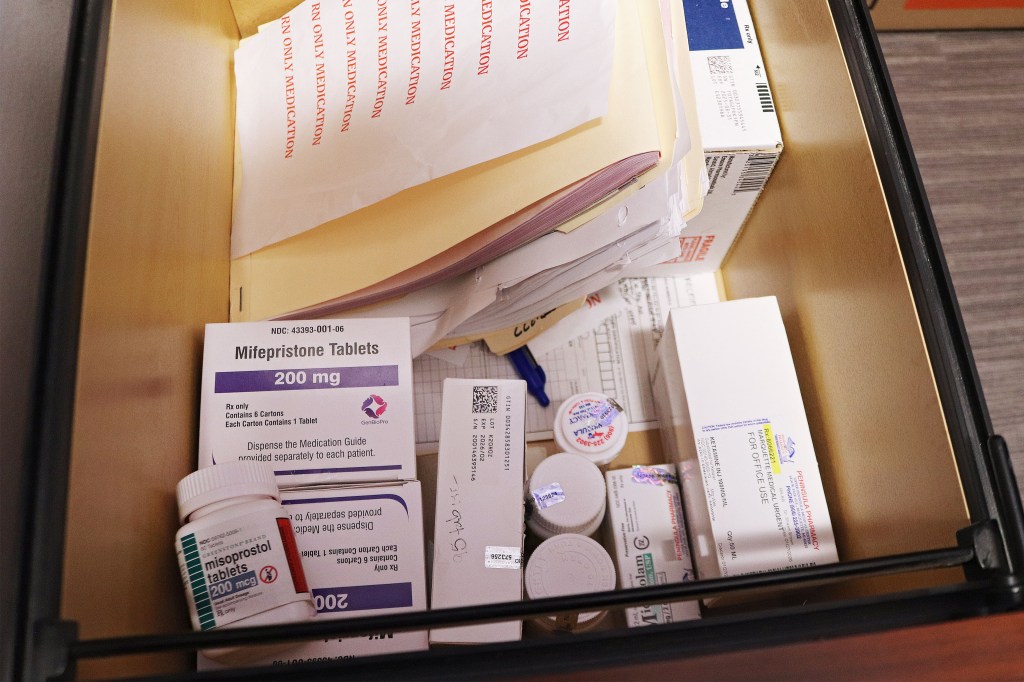
The Urgent Care Option
The options presented at that community clubhouse meeting were limited. The few family medicine doctors and OB-GYNs in the area were either already putting patients on months-long waitlists or were too “rightward leaning,” Brown said.
But urgent cares are designed to fill gaps in the system, she said, ready to take walk-ins who aren’t already patients.
Brown knew from her years in the emergency room that medication abortions aren’t that complicated. The professional guidelines for first-trimester medication abortions and miscarriages are essentially the same: one dose of mifepristone, followed by misoprostol after 24 to 48 hours.
“Clinically, I was never worried about it,” she said.
The biggest hurdle was getting medical malpractice insurance, Brown said. At first, insurers balked, demanding “onerous and unrealistic” documentation and additional training, she said. Then they quoted a $60,000 annual premium for medication abortions — about three times the cost of insuring the entire urgent care. Ultimately, Brown said, the urgent care’s broker pushed back, providing data that medication abortions didn’t add “significant liability.”
The company agreed to a premium of about $6,000 per year, she said.
The community pitched in, too. A local donor covered an ultrasound machine. And supporters started a nonprofit to help pay for the costs of the medication and additional staffing, bringing the price for patients down from about $450 to an average of about $225, based on a sliding scale.
Word spread quickly once Marquette Medical began offering medication abortions, Brown said. Now the office provides as many as four per week, with patients traveling from as far away as Louisiana. The clinic is on track to match the volume of abortion patients treated at the local Planned Parenthood office before its closure, Brown said.
As pills by mail become the next major target for abortion opponents, Chernoby said, it will be critical to offer more care in more brick-and-mortar places. Brown said the Marquette clinic has already fielded questions from a large academic medical center that plans to start providing medication abortion at its own urgent cares later this year.
“It’s a wonderful idea, but it’s potentially got major pitfalls,” said David Cohen, a professor at the Drexel University Kline School of Law who studies abortion access.
Urgent cares that provide medication abortion would have to abide by state-specific laws — some mandate 24-hour waiting periods or facility structural requirements — and federal regulations, such as the FDA’s requirement that mifepristone prescribers be certified by the drug’s distributors and obtain signed patient agreements.
If abortion access isn’t a core part of a health organization’s mission, “do you want to be on that list? I don’t know if you do,” Cohen said. “There’s just a very particular regulatory environment” around abortion.

Making a Choice
In the exam room, Koskenoja listened as A talked about why she decided to seek an abortion. She has four kids at home, including the baby.
“You OK if we do an ultrasound, just confirm how far along you are, make sure it’s not an ectopic pregnancy?” Koskenoja asked.
“Yeah,” A said.
Koskenoja noted A’s reaction to the question. “OK. You’re making a face?”
“Yeah, I just don’t — yeah, it’s fine. I just don’t want to see it.”
“Oh, you don’t have to see it,” Koskenoja said.
“I just don’t want to hear a heartbeat or anything like that,” A said.
“Definitely not,” Koskenoja said.
After the ultrasound, Koskenoja stepped out into the hall to give A time to call her partner.
When A said she was ready, Koskenoja stepped in and asked her how she was feeling. A had made up her mind. She said that her partner would be supportive of whatever she decided and that she didn’t want to have another baby right now.
“As much as I know this baby would be loved no matter what, it’s just not a good time,” A said quietly, her hands in her lap.
“Most people who get abortions love babies,” Koskenoja said. And you can still have more in the future, she assured A.
This kicked off a long conversation about the mental load of parenting and the pros and cons of various birth control options. A said she wanted to get her tubes tied, but Koskenoja suggested her partner consider a vasectomy instead. It’s a much less invasive procedure, she said. “You’ve had a lot of kids. I feel like it could be his turn to take some responsibility.”
Koskenoja handed her a small, handsewn “comfort bag” that all medication abortion patients receive. It was filled with the pills, reminders about when to take them, a handwritten note of support from local community members, pain meds, comfortable socks, and a heating pad.
“Call us if you need anything,” she told A. “Any questions?”
“No,” A said.
“OK. Good luck,” Koskenoja said before A walked out past the waiting room, filled with sick babies and other patients, to drive back to her kids.
This <a target="_blank" href="https://kffhealthnews.org/health-care-costs/abortion-providers-clinics-closing-urgent-care-michigan-upper-peninsula/">article</a> first appeared on <a target="_blank" href="https://kffhealthnews.org">KFF Health News</a> and is republished here under a <a target="_blank" href="https://creativecommons.org/licenses/by-nc-nd/4.0/">Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="https://kffhealthnews.org/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="https://kffhealthnews.org/?republication-pixel=true&post=2174428&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>A mom of seven, Pipe is a doula on the reservation who supports new and expectant parents. She does that work free, around her day job. That’s because in this town of about 2,000 people, the closest hospital that delivers babies is 100 miles away.
“Women need this help,” Pipe said.
Doulas ready parents for childbirth, support their deliveries, and can be a steady presence in a baby’s first months. Studies link their work with lower rates of costly birth and postpartum complications — especially in hard-to-reach places like Lame Deer.
But that help can be scarce. As Pipe put it: “Doula doesn’t pay the bills around here.”
Things were supposed to change this year. Montana was set to join at least 25 other states that reimburse doulas through their Medicaid programs to ease gaps in care. Montana lawmakers approved the payments last year, authorizing up to $1,600 per pregnancy. Pipe hoped that money would give her the chance to leave her post office job one day to help more parents.
But the state Department of Public Health and Human Services postponed adding doula services to its Medicaid program in late March, citing a budget shortfall driven in part by higher-than-expected Medicaid costs.
“DPHHS will not be moving forward with the implementation of doula services in the Montana Medicaid benefit package at this time,” department spokesperson Holly Matkin told KFF Health News.
The news caught Pipe by surprise — she hadn’t heard any updates in a while, but the state had finalized its licensing rules for doulas in January. Last year, she supported three people through their deliveries. She doesn’t have time for much more. That weighs on her. Nearly half the people on the Northern Cheyenne Indian Reservation live in poverty, and the people she helps usually can’t afford to pay a doula.
“I was looking forward to serving more people,” Pipe said. “Now that’s not going to happen anytime soon.”


Charlie Brereton, who heads the health department, told state lawmakers in March that the agency projected a $146.3 million shortfall in federal Medicaid funds for this year. Health officials predict another deficit next year as states feel the effects of Republicans’ massive tax-and-spending law, the One Big Beautiful Bill Act. Signed last year, that law is projected to reduce federal Medicaid spending by nearly $1 trillion over 10 years.
Matkin said it’s “unclear” whether the agency can authorize doula coverage this year. The deficit will lead the department to seek supplemental funding from state lawmakers. When an agency makes that kind of request for the first year of the state’s two-year budget cycle, Montana law requires it to create a plan to reduce its spending.
Around the country, optional Medicaid services — such as doula support, home health care, and dental work — are at risk of losing funding as states brace for federal Medicaid cuts to hit their bottom lines. Already, lawmakers in Idaho are considering their own reductions to Medicaid to balance the state’s budget. Missouri officials proposed cutting tens of millions of dollars in services for people with disabilities.
In Montana, doula services are unlikely to be the only Medicaid cutbacks announced. “All options are on the table,” Brereton told lawmakers in March.
Stephanie Morton, executive director of Healthy Mothers, Healthy Babies-The Montana Coalition, said more than half of Montana’s counties are designated as maternity care deserts.
“Budget cuts will continue to diminish the limited services families rely upon in these counties,” said Morton, whose nonprofit had advocated for doula Medicaid reimbursement. “This decision feels like the first of many rollbacks and cuts Montanans will face.”
Laboring Alone
At the check-in just outside town, Pipe handed a waking newborn to his mother and unwrapped a new swaddle for the child. This would have to be a quick visit — she was already late for work.
The mother, Britney WolfVoice, held her newborn son as her three young daughters stood close by. Pipe has been with WolfVoice and her husband for the birth of their newborn son and youngest daughter.
She helped them create delivery plans. For the birth of WolfVoice’s youngest daughter a few years ago, Pipe brought cedar oil, a sacred plant used for prayer, and calmed WolfVoice through her contractions. For the recent birth of her son, when hospital backlogs delayed WolfVoice’s induction, Pipe encouraged her to advocate for an earlier appointment by routinely calling the hospital. Doctors had recommended the procedure to avoid complications.
“Misty is one person who I can count on to be my voice,” WolfVoice said.
If someone needs a ride to a doctor’s appointment, Pipe takes time off work to drive them. If a client goes into labor when Pipe’s at the post office, she texts two other free doulas she knows of on the reservation to see if they have time to help until her shift ends. But they also have day jobs.
Pipe herself has ridden that 100-mile stretch between home and the hospital in labor and in the back of an ambulance. Twice, she gave birth in emergency rooms along the way. In one of her pregnancies, she miscarried at home and couldn’t get a doctor appointment for days.
The long distance to receive care often meant her husband had to stay behind to tend to their other children at home.
“I labored alone so many times,” Pipe said. “I just want to make sure no one’s alone.”

Rural maternity care deserts are a national problem, especially as labor and delivery units continue to shutter. In many tribal communities, a lack of care coincides with long-standing inequities caused by centuries of systematic discrimination.
Predominantly Indigenous communities face the longest distances to obstetric facilities compared with all other racial and ethnic groups, according to a 2024 report from the March of Dimes. That’s part of the reason Indigenous women are far more likely to get sick from pregnancy and at least twice as likely to die as white women.
Indigenous patients are supposed to be guaranteed access to health care through the federal Indian Health Service. But the chronically underfunded agency has severe gaps. A small fraction of its hospitals and clinics offer labor and delivery. As of 2024, only seven states had either an IHS or tribal birth facility, the agency reported. To help fill in those shortfalls, Medicaid is the main source of health coverage for many Native Americans, according to KFF.
Even where care exists, Native women can experience a distrust of health systems, according to Pipe and other health workers. The U.S. government has a long history of removing children from tribal homes and forcing Native American women to undergo sterilization.
Emily Haozous of the Pacific Institute for Research and Evaluation’s Southwest center has studied premature deaths among Native Americans. A member of the Fort Sill-Chiricahua-Warm Springs-Apache Tribe, Haozous said data on maternal health disparities in pregnancy and postpartum often misses a key point.
“It’s not that women are just not taking care of themselves,” Haozous said. “The system is set up for them to not have access to care.”

On top of funding cuts, the One Big Beautiful Bill Act will add more frequent eligibility checks and work requirements to access Medicaid. Those changes, when they take effect later this year and next, will lead an estimated 5.3 million people to lose their coverage by 2034.
Native Americans are exempt from some of the law’s new rules, such as the work requirements. Even so, tribal patients can get tangled in administrative hurdles. That includes struggling to enroll in the first place or to prove their tribal status. A full-time college student, WolfVoice said that when she got pregnant, it took about six months to enroll in the state’s Medicaid program.
Despite Montana’s long struggle with a backlogged Medicaid system, state officials aim to implement work requirements this summer, well before the federal deadline.
‘Moccasins on the Ground’
As Pipe pulled into her driveway one day after a full shift at the post office, her kids ran to her. She was also greeted by Felicia Blindman, a 63-year-old public health nurse who used to work for the tribe. The two sat in lawn chairs into the night and brainstormed ways to connect more women to services — such as free prenatal classes.
Pipe’s four youngest children played around them. Her 14-year-old daughter is already certified as an Indigenous doula. Her 8-year-old daughter has begun helping Pipe pick up prescriptions for moms without a car who live out of town. Pipe hopes one day they could do that work full-time, if they want to.
Because of the lost Medicaid payment, Pipe said, she will continue to balance her job with her birth work, even if it means persuading more people to become doulas, such as family and respected community members, to cover more ground.
“It’s not going to stop me from training more birth workers, more young people, more aunties,” Pipe said. “For now, I guess it’s more about grassroots, moccasins on the ground, helping each other.”
She said that means telling pregnant people who walk into the post office she’s there to help if they need support. At least, as long as she’s not at her day job.

This <a target="_blank" href="https://kffhealthnews.org/health-care-costs/doula-care-indigenous-health-medicaid-cuts-montana-tribe/">article</a> first appeared on <a target="_blank" href="https://kffhealthnews.org">KFF Health News</a> and is republished here under a <a target="_blank" href="https://creativecommons.org/licenses/by-nc-nd/4.0/">Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="https://kffhealthnews.org/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="https://kffhealthnews.org/?republication-pixel=true&post=2176418&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>