They discussed the pivotal role the president of the United States plays in health policy — whether it is building support for or opposition to new plans and proposals. “Presidents have a level of authority which is often underappreciated, especially in health care,” Blumenthal said.
Blumenthal and Rovner also discussed the historical reasons the U.S. has been unable to enact universal health care, incrementalism versus sweeping change, and what he described as “the dance” between proponents and opponents — usually a clear party-line split between Democrats and Republicans — of major health care reforms.
Today, the split seems to have come to a head, as public health, science, and expertise are being viewed by one end of the political spectrum as “the opposition,” Blumenthal said, which will complicate efforts. Still, he outlined ideas for moving forward.
An abbreviated version of this interview aired April 23 on Episode 443 of What the Health? From KFF Health News: “RFK Jr. vs. Congress.”
Blumenthal’s latest book, Whiplash: From the Battle for Obamacare to the War on Science, co-written with James A. Morone, offers a behind-the-scenes look at how three presidential administrations pursued very different health policy goals.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.This <a target="_blank" href="https://kffhealthnews.org/health-industry/health-care-policy-political-divide-david-blumenthal-interview/">article</a> first appeared on <a target="_blank" href="https://kffhealthnews.org">KFF Health News</a> and is republished here under a <a target="_blank" href="https://creativecommons.org/licenses/by-nc-nd/4.0/">Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="https://kffhealthnews.org/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="https://kffhealthnews.org/?republication-pixel=true&post=2230749&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>{kind=link}

President Donald Trump this week nominated a former deputy surgeon general who has expressed support for vaccines to lead the Centers for Disease Control and Prevention. Considered a more traditional fit for the job, Erica Schwartz would be the agency’s fourth leader in roughly a year, should she be confirmed by the Senate.
And Health and Human Services Secretary Robert F. Kennedy Jr. appeared on Capitol Hill this week in the first of several hearings discussing Trump’s budget request for the department. But the topics up for discussion deviated quite a bit from the subject of federal funding, with lawmakers raising issues of Medicaid fraud, measles outbreaks, the hepatitis B vaccine, peptides, unaccompanied minors, and much, much more.
This week’s panelists are Mary Agnes Carey of KFF Health News, Anna Edney of Bloomberg News, Emmarie Huetteman of KFF Health News, and Joanne Kenen of the Johns Hopkins University Bloomberg School of Public Health and Politico Magazine.
Panelists



Among the takeaways from this week’s episode:
- Trump on Thursday named four officials to the CDC’s leadership team. Schwartz, whom he picked as director, is a physician and Navy officer who served as a deputy surgeon general during Trump’s first term. She has voiced support for vaccines and played a key role in the covid-19 pandemic response.
- RFK Jr. testified before three committees of the House of Representatives this week on the president’s budget request for HHS. While the hearings touched on a wide variety of topics, notable moments included a slight softening of Kennedy’s stance on the measles vaccine, including the acknowledgment that being immunized is safer than having measles — although he also stood by the decision to remove the recommendation for the newborn dose of the hepatitis B vaccine.
- New studies on the use of acetaminophen during pregnancy and the effects of water fluoridation on cognitive function refute Trump administration claims. And a White House meeting that brought together Trump, Kennedy, and other leaders of the Make America Healthy Again movement aimed to soothe concerns among supporters — yet there’s reason to believe the overture won’t completely mend fences between the Trump administration and the MAHA constituency ahead of the midterm elections.
Also this week, KFF Health News’ Julie Rovner interviews Michelle Canero, an immigration attorney, about how the Trump administration’s policies affect the medical workforce.
Plus, for “extra credit,” the panelists suggest health policy stories they read (or wrote) this week that they think you should read, too:
Mary Agnes Carey: Politico’s “‘A Crisis in the Making’: Nebraska Races To Impose Work Requirements on Medicaid,” by Alice Miranda Ollstein.
Joanne Kenen: The New York Times’ “He Warned About the Dangers of A.I. If Only His Father Had Listened,” by Teddy Rosenbluth.
Anna Edney: Bloomberg’s “Hormone Drugs Make $6.3 Billion Comeback After FDA Nixes Safety Warnings,” by Anna Edney.
Emmarie Huetteman: KFF Health News’ “Your New Therapist: Chatty, Leaky, and Hardly Human,” by Darius Tahir.
Also mentioned in this week’s podcast:
- JAMA Pediatrics’ “Acetaminophen Exposure During Pregnancy and the Risk of Autism in Offspring,” by Kira Philipsen Prahm, Pingnan Chen, Line Rode, et al.
- Proceedings of the National Academy of Sciences’ “Municipal Water Fluoridation, Adolescent IQ, and Cognition Across the Life Course: Evidence From the Wisconsin Longitudinal Study,” by John Robert Warren, Gina Rumore, Kamil Sicinski, and Michal Engelman.
- KFF Health News’ “Pennsylvania Town Faces Fallout From Trump’s Environmental Rule Rollback,” by Stephanie Armour and Maia Rosenfeld.
- The New York Times’ “In Private Meeting, Trump Soothes Disenchanted MAHA Leaders,” by Sheryl Gay Stolberg.
- Wakely Consulting Group’s “Who Paid, and Who Stayed? Early 2026 Enrollment Trends in the Individual Market,” by Michelle Anderson, Chia Yi Chin, and Michael Cohen.
[Editor’s note: This transcript was generated using both transcription software and a human’s light touch. It has been edited for style and clarity.]
Mary Agnes Carey: Hello from KFF Health News and WAMU radio in Washington, D.C. Welcome to What the Health? I’m Mary Agnes Carey, managing editor of KFF Health News, filling in for Julie Rovner this week. And as always, I’m joined by some of the best and smartest health reporters covering Washington. We’re taping this week on Friday, April 17, at 10 a.m. As always, news happens fast and things might have changed by the time you hear this. So here we go.
Today we’re joined via videoconference by Anna Edney of Bloomberg News.
Anna Edney: Hi, everybody.
Carey: Joanne Kenen of the Johns Hopkins Bloomberg School of Public Health and Politico Magazine.
Joanne Kenen: Hi, everybody.
Carey: And my KFF Health News colleague Emmarie Huetteman.
Emmarie Huetteman: Hey there.
Carey: Later in this episode, we’ll play Julie’s interview with immigration attorney Michelle Canero about the impact the Trump administration’s immigration policies are having on the medical workforce. But first, this week’s news — and there is plenty of it.
On Thursday, President [Donald] Trump nominated Dr. Erica Schwartz to lead the Centers for Disease Control and Prevention. Schwartz, a vaccine supporter, served as a deputy surgeon general in President Trump’s first term, and during the coronavirus pandemic she ran the federal government’s drive-through testing program. She’s also a Navy officer and a retired rear admiral in the Commissioned Corps of the U.S. Public Health Service. Her appointment requires Senate confirmation. President Trump also announced other changes to the agency’s top leadership: Sean Slovenski, a health care industry executive, as the agency’s deputy director and chief operating officer; Dr. Jennifer Shuford, health commissioner for Texas, as deputy director and chief medical officer, and Dr. Sara Brenner, who briefly served as acting commissioner of the FDA [Food and Drug Administration], as a senior counselor to Department of Health and Human Services Secretary Robert F Kennedy Jr. So we’ve discussed previously on the podcast several times that the CDC has lacked a permanent director for most of the president’s second term. Will Dr. Schwartz, if confirmed, and the other members of this new leadership team make the difference?
Huetteman: I think that we’ve seen a CDC that’s been in a protracted period of turmoil, and this is going to be an opportunity for maybe a shift in that. Dr. Schwartz would actually be the agency’s fourth leader in a little more than a year, and we’ve talked on the podcast about how naming someone who could fit the bill to lead the CDC was a difficult task facing the Trump administration. They needed someone who could support the MAHA [Make America Healthy Again] agenda while not embracing some of the more anti-vaccine views, and that person needed to be able to win Senate confirmation, which isn’t a given, even with this Republican-controlled Senate.
Edney: And I think we’ve seen that there have been some people already in the MAHA coalition that have come out and been upset about this pick. So I think what that shows is a calculated decision by the administration to, kind of, as they’ve been doing for this year, is kind of not focus on the vaccine part of Secretary Kennedy’s agenda and to, as Emmarie said, try to get someone that can get through Senate confirmation. We’ve already seen the surgeon general nominee be held up in the Senate because she was not as strong on vaccines as I think some would have liked to see when she had her confirmation hearing.
Kenen: So this happened late yesterday, and I’ve been traveling this week, but I did have a chance to talk to some public health people about her, and there was sort of this audible sigh of relief. The Senate is a very unpredictable place, and we live in very unpredictable times. At this point, my initial gut reaction is she’s got a pretty good chance of confirmation. The other thing, I think some of the other appointees, there’s a little bit more concern about, but what really matters is who is the face of the CDC, and she would be the face of the CDC. She would be in charge, and people like her. Also, this is an administration that has not had a lot of minorities, and she will be, she’s a Black woman. respected in her field. And that also is going to — she needs to be able to speak to all Americans about their health, and I think that people welcome that as well, both her credentials and her life experience. So, yeah, I think that MAHA is sort of in this funny moment now, because clearly Kennedy isn’t doing everything that people wanted or expected. And so we’ll sort of see how the — I think if he had his ideal CDC director, this, we can probably surmise that this would not, she would not be the first on his list. But there’s a certain amount of adaptation going on at the moment. So I think many, many people will be relieved to see somebody get through, confirmed pretty quickly. People can get held up for things that have absolutely nothing to do with the CDC or public health. The Senate has all sorts of peculiarities. But I think there’s probably going to be a desire to get this done pretty quickly.
Carey: All right. Well, we’ll see what happens, and we will go back to the MAHA folks a little bit later in the podcast. But right now I want to shift to Capitol Hill. Thursday was a very big day on the Hill for HHS Secretary Kennedy. He kicked off a series of appearances before Congress. This week he’s testifying before three House committees before he heads over to the Senate next week. This is the first time that the secretary has visited some of these House panels, and while the purpose of the latest congressional visit is to talk about President Trump’s HHS budget request, this also was the first time that a lot of lawmakers ever had an opportunity to talk to Kennedy, and what they asked him sometimes deviated, maybe quite a bit, from that subject of federal funding. The topics included Medicaid fraud, measles outbreaks, the birth-dose recommendation for the hepatitis B vaccine, peptides, unaccompanied minors, and more — actually, much more when you look at the hearings from yesterday, and I’m sure that will also happen with today’s session. What stood out to you about Kennedy’s testimony this week?
Edney: I think it was the mix of questions, and you sort of alluded to this, but they wanted, the members of Congress wanted to talk about so many things. And I feel like in the earlier hearing, which was in the House Ways and Means Committee, that it was, there was a lot of focus in the beginning on fraud, and that sort of surprised me, and then we saw maybe one or two questions on vaccines. And so I thought the mix of questions, the things that members were interested in, were really interesting. And it did — there were some fiery moments, but for his first time on the Hill in a while, for such a controversial Cabinet member, I thought they were pretty tame.
Kenen: Yeah, I watched a fair amount of the morning. I did not see the afternoon, but I read about the afternoon, and I totally agree with Anna’s take. This administration and Kennedy did what this administration has been doing. They blame all problems on [former president Joe] Biden and the prior administration. And to be fair, Democrats, when they’re in power, they, I don’t think they do it quite to this extreme, but Democrats spend, when they have the chance, they blame things on Republicans. So that’s sort of Washington as usual. The emphasis on fraud has been a hallmark of this administration, particularly in health and social services. And you’ve seen, of course, in the way they’ve gone after blue states in particular. And a lot of their justification for the changes in Medicaid that are coming in the coming year are supposedly because of massive fraud and they’re cracking down. It was not dominated by vaccines, and I was watching Kennedy’s face really carefully. When he was asked about the first child to die of measles in Texas last year, and a Democrat asked him could the vaccine have saved her life, and you could sort of see him just, you just sort of watch his facial expressions, and he knew he had to say this, and he came out with the word “possibly,” and, which is a change. And then in the afternoon — where I did not, as I said, I did not watch the afternoon, but I read about it — he was much more certain. He was much stronger about the measles vaccine and said it’s, the measles vaccine, is safer than measles, which is a big signal shift there.
Huetteman: It’s true, although I will point out, though, that he did stand by the decision to remove the recommendation for the birth dose of the hepatitis B vaccine when he was pressed on that. So it was, I agree it was a softening, I’d say. At least it wasn’t a dramatic turnaround from what he’d said or not said in the past. But for him, it was at least a softening.
Kenen: In the hepatitis B recommendation, he said that the biggest threat to infection was at, through birth, at, through the mother, and if you test the mother, the baby is not at risk. And that’s partially true, and that is a significant factor to eliminate risk. It doesn’t — it minimizes risk. It does not eliminate risk. Babies can and have been infected in the first weeks of life in other ways. The recommendation was not to totally eliminate that vaccine. It was to postpone it. But there’s, public health, still believe that, in general, many public health leaders would still say that the vaccine at birth is the better way of doing it.
Carey: The focus was, theoretically, on the budget request from the administration. Did the secretary shed any light on those priorities or their impacts? I was taken, I think in the afternoon hearing I read about various lawmakers, including Rosa DeLauro from Connecticut, who sort of just said: A CDC cut of 30%? We’re not gonna do that. And there were also some Republican members who jumped in to sort of say, I don’t think we’re going to do the cuts you envision. But did the secretary defend them? Did he bring any new clarity to them?
Edney: I don’t feel like I gained any new clarity on it. I think to bring it back to Budget 101, I guess, is like when the president, when the administration, sends down their budget, I think a lot of people already assume it’s dead on arrival. And maybe even though Kennedy is there to talk about the budget, it does become this broader hearing, because they don’t get him on the Hill that often and people go there to talk about all kinds of things, and I think that he probably knew that he didn’t have to defend it in the same way, because it’s not going to happen.
Carey: Sure. As they say, the president proposes and Congress disposes. But Joanne, you want to jump in?
Kenen: Yeah, there’s something significant about this administration, which is Congress has repeatedly authorized more money for various health programs and science programs, and the administration doesn’t spend it, so that there’s a different dynamic. Traditionally, yes, Congress — the president proposes, Congress legislates, and then people go off and spend money. That’s what people like to do. And in this case, when Congress has, in a bipartisan way, differed with the administration and restored funding, it hasn’t all gone, those dollars haven’t gone out the door. So the entire sort of checks-and-balances system has been askew in terms of funding. I agree with everybody here. I do not think that Congress is going to accept these extreme cuts across the board in health care and health policy, in public health and science and NIH [the National Institutes of Health] and everything, but I don’t know what they’re actually going to spend at the end of the day.
Carey: Emmarie, you wanted to jump in.
Huetteman: Yeah, there was one striking exchange to me where the secretary acknowledged he wasn’t happy with the cuts that were proposed. I think those were his words. But he pretty quickly added, and neither is President Trump, and he framed it as a matter of making hard decisions when faced with federal budget shortfalls.
Carey: All right. Well, we’ll keep watching this as it moves through Congress. Also during yesterday’s House Ways and Means hearing, some Democrats took issue with past statements from Secretary Kennedy and President Trump that linked Tylenol use during pregnancy to autism in children. A new study released this week in JAMA Pediatrics found that the use of Tylenol by women during pregnancy was not associated with autism in their children. This nationwide study from Denmark followed more than one and a half million kids born between 1997 and 2002, including more than 31,000 who were exposed to Tylenol in the womb. A separate study in another medical journal examining community water fluoridation exposure from childhood to age 80 found no impact on IQ or brain function. Kennedy has claimed that fluoride in water has led to IQ loss in children. These studies clearly debunk medical claims that have gotten a lot of attention. Will these findings have an impact now?
Kenen: I think we’ve seen over and over and over again that there are people who are very deeply wedded to certain beliefs, and new science, new research, does not deter them from those beliefs. We also see some people who are sort of in the middle, who are uncertain, and new findings can shift their beliefs, right? And then, of course, there’s a lot of — these are not new studies. I mean these are new studies but they are not the first of their kind. The reason we’ve been using fluoride for, what, 60 years now in the water. Tylenol has been around a long time. So is it going to change everybody’s belief? No. Is it going to perhaps slow the push to ban fluoridation? Perhaps. But I just don’t think we know, because we’re sort of on these dual-reality tracks regarding a lot of science in this country, where once people sort of buy into disinformation, they’re very, it’s very hard to change — or misinformation — it’s hard to change people’s minds.
Edney: I do think, on the Tylenol front — I absolutely agree with what Joanne said overall. And I think on the Tylenol front that it’s possible that this study will give pediatricians something to give and talk about with parents that are asking. I think there still is some confusion among some people. It’s not a huge, I don’t think, widespread thing, but I think there are some new parents who are wondering. And if you are able to take this study that is published in 2026 — it just happened, it was after Trump made his statements — I think maybe that would give them something to talk about with their patients.
Kenen: I agree with Anna. I think the Tylenol one is easier to change than some of the fluoridation stuff going on, partly because so many of us — and we should just say, it’s not just the Tylenol, the brand. It’s acetaminophen, which I’ve never pronounced right. I think those of us who have been pregnant, we’ve taken that in our life before and we don’t think of it as a big, dangerous, heavy prescription drug. I think we’ve, it’s something we feel comfortable with. And I think there’s also the counterinformation, which is, a fever in a pregnant woman can, a pregnant person can be dangerous to the fetus. So I think that one’s a little — and I don’t, also, I don’t think it’s as deep-rooted. The fluoridation stuff goes back decades, and the Tylenol thing is sort of new. And it might be, I’m not sure that the course of these arguments — I think that Tylenol is easier to counter than some other things, because partly just we do feel safe with it.
Carey: All right. We’re going to take a quick break. We’ll be right back.
We’re back and talking about how the Trump administration is managing the voters behind the Make America Healthy Again, or MAHA, movement, which helped President Trump win the 2024 election. My colleagues Stephanie Armour and Maia Rosenfeld wrote about the administration’s recent decision to give coke oven plants in the U.S. a one-year exemption from tougher environmental standards. And that was a move that angered some MAHA activists who wondered if the GOP is more beholden to industry than the MAHA agenda. President Trump, HHS Secretary Kennedy, and other top administration officials met recently at the White House with a group of MAHA leaders to calm concerns that the administration is moving too slowly on food policy changes, and they are concerned about the president’s recent support of the pesticide glyphosate. According to press reports, the MAHA folks seem to feel their concerns were heard during that session. But is this ongoing conflict between the president and this key political constituency, will it be one that keeps brewing as the midterm elections approach?
Edney: Yes, 100%. I think it will continue to brew. I think that meeting was thrown together so quickly that some members of the MAHA movement who were invited couldn’t even make it. So it wasn’t exactly a long-planned, seemingly deep desire to fix everything. But it was, as you’ve said, an effort to kind of hear them out and make them feel heard. No one that I’ve talked to has said everything is fixed now. It’s more of a to-be-determined We will see what the administration will do moving forward, if they will listen to any of our plans — which we will not share with you, by the way — to make us happy. And I think that that’s going to continue. There’s a rally planned in front of the Supreme Court on glyphosate later this month where a lot of those people will be, and so I think that they’re upset and they’re stirring up, that concern is only going to get stirred up more.
Carey: Emmarie.
Huetteman: It’s a small thing, but our fellow podcast panelist Sheryl Stolberg at The New York Times reported that during this White House meeting where President Trump was meeting with MAHA leaders, one of the leaders made a joke about how this is not a group that’s going to be, quote, “Team Diet Coke,” and the president apparently took that as a cue to press that Diet Coke button he famously has on his desk and summon a server who apparently brought him a Diet Coke. Supporters of MAHA have been clear that they want not just for the Trump administration to promote policies supporting priorities like healthy eating and removing food dyes, but also they want them to rein in or end policies they don’t support. And that weed-killer executive order, that really was a big example of that. The MAHA constituency made it clear that they felt betrayed by that order, and they’re going to have to do some work to walk that back.
Carey: We’ll also see how, with their concerns about the new CDC director nominee, which they’re already voicing, we’ll see how that plays out.
Kenen: No, I just think that we are, as we mentioned at the beginning, we’re seeing cracks, right? We’re seeing — none of us are privy to any conversations that President Trump has had privately with Secretary Kennedy. But his, Secretary Kennedy’s, public statements have been a little different than they were a few months ago. There’s certainly been reports that he’s been told to soft-pedal vaccines and talk about some of the things that there’s more unanimity across ideological and party lines. Healthier food — there’s debate about how to, whether, there’s debate about how Kennedy defines healthier food. But in general, should we eat healthier? Yes, we should eat healthier. Should our kids get more exercise? Yes, our kids should get more exercise. Do we have too much chronic disease? Yes, we have too much chronic disease. So they’re sort of this, trying to move a little bit more, sort of this sort of top line, very hazier agreement. But at the same time, the people who are sort of really the core of MAHA, as Kennedy has sort of created it or led it, there’s cracks there.
Carey: All right, we’ll see. We’ll see where that goes. But let’s go ahead and move on to ACA enrollment. A new report found that 1 in 7 people who signed up for an Affordable Care Act plan failed to pay their first month’s premium. The analysis from Wakely consulting group found that nationally around 14% of those who enrolled in ACA plans didn’t pay their first bill for January coverage. Now we know the elimination of the enhanced ACA tax credits and higher premium costs led to lower enrollment in the ACA exchanges, with sign-ups for 2026 falling to 23 million from 24 million a year ago. But how do you interpret this finding that 14% of enrollees didn’t pay their January premium? Is it a sign of more trouble ahead?
Edney: I think it could be a sign of more trouble ahead. Some — what we’re seeing is sticker shock. And there may be some people who are trying to deal with that and won’t be able to as the months go on. And so, yeah, I think it could mean that even more drop out, and that means more people lose coverage and are uninsured.
Kenen: I think there was sort of a general, initial, misleading sigh of relief when in December, when the enrollment figures, the drop wasn’t as bad as some feared. But at the same time, people said: Wait a minute. This doesn’t really count. Signing up isn’t the same thing as staying covered. The drop in January was significant, we now know. And I agree with Anna. I think we don’t know how many more people will decide they can’t afford it. Or we don’t know whether the big drop is January. Probably a lot of it is, because you get that first bill. But can, will more people drop? Probably. We have no way of knowing how many. And it also depends on the economy, right? If more people lose jobs, right now it’s still pretty, kind of still pretty stable, but we don’t know what’s ahead. We don’t know what’s going to happen with the war. We don’t know many, many, many — we don’t know anything. So the future is mysterious. I would expect it to drop more. I don’t think, I don’t know whether this is the big drop or February will be just as bad. I suspect January will be the biggest. But who knows? It depends on other outside factors.
Huetteman: We’re also seeing a drop-off in the kind of coverage that people are choosing. That analysis that you referenced, Mac, showed that there was a 17% drop in silver plan membership, with most of those folks switching to bronze plans, which, in other words, that means they switch to plans that have lower monthly premiums but they have higher deductibles. And that means that when you get sick, you owe more, in some cases much more, before your insurance starts picking up the tab. And I think really what this means is people are more exposed to the high charges for medical services, bigger bills when you get sick. I think that
Kenen: I think that the Republicans were seen as having pushed back a lot of the health impacts of the so-called One Big Beautiful Bill and that it would be after the election. And I and others wrote: No, no, no, no, no. We’re going to see this playing out before the election. This is a really big political red flag, right? This is a lot more people becoming uninsured, which makes other people worried about their insurance and stability. So I think this is definitely going to — it may not be. There are other things going on in the world. Health care may not be the dominant theme in this year’s election. But yes, this is going to be, the off-year elections are going to be health care elections, like almost every one else has been for—
Carey: Oh yeah.
Kenen: —since the Garden of Eden, right?
Carey: Absolutely, it’s a perennial. All right, we’ll keep our eye on that. That’s this week’s news. Now we’re going to play Julie’s interview with immigration attorney Michelle can arrow, and then we’ll be back with our extra credits.
Julie Rovner: I am pleased to welcome to the podcast Michelle Canero. Michelle is an immigration attorney from Miami and a member of the board of Immigrants’ List, a bipartisan political action committee focused on immigration reform. Michelle, thanks for joining us.
Michelle Canero: Thank you for having me.
Rovner: So, we’ve talked a lot about immigration policy on this podcast over the past year, but I want to look at the big picture. How important to the U.S. health care system are people who originally come from other countries?
Canero: I think the statistics speak for themselves. One in three residency positions can’t be filled by American graduates alone. That means 33% of these residency positions are being filled by immigrant workers. Twenty-seven percent of physicians are foreign-born. Twenty percent of hospital workers are immigrants. And, at least in Florida, a large percentage of our home health care workers happen to be immigrants. And we depend on this population heavily in the health care sector.
Rovner: Now, we talk a lot about the Trump administration’s crackdown on illegal immigration, but we talk a little bit less about their sort of messing with the legal immigration system. And there’s a lot going on there, isn’t there?
Canero: There is. And I think that the campaign talking points were illegal immigration but what we’re actually seeing is a little more sinister. I think that the goal of leadership at the head of DHS [the Department of Homeland Security] and DOS [the State Department], or really Stephen Miller, is pushing something called reverse migration, which is really not about limiting illegal immigration but reducing the immigrant population in the United States. And I think that’s where the real concern is and why you’re seeing these policies that directly affect legal immigrants.
Rovner: We talk a lot about doctors and nurses and skilled, the top skilled, medical professionals who make up a large chunk of the United States health care workforce. We don’t talk as much about the sort of midlevel professional workers and the support staff. They’re also overwhelmingly immigrant, aren’t they?
Canero: Yeah, and whether it’s your IT- and technical-knowledge-based workers in hospitals who facilitate all the technology — we rely on an immigrant workforce for a lot of the technology sector. And then you’ve got research professionals. A lot of clinical researchers, medical researchers, are foreign-born. So it’s not just about the doctors. It’s also the critical staff that keep the hospitals operating. And I’m from Florida. For us, it’s the home health care workers. We have an aging population, and a large percentage of the home health care workers, particularly in Florida, happen to be Haitians on TPS [temporary protected status] or people with asylum work authorizations. And when we lose that, our aging population is left with no resources, because that’s not something AI or technology can fix. You can’t turn someone over in a bed with a robot yet, and we’re probably decades away from that.
Rovner: So what’s the last year been like for you and your clients?
Canero: I think it’s a lot of uncertainty. A lot of these policies are percolating, and we’re assuming that they’ll be resolved in litigation, but the damage is being done in real time. So we’re seeing hospitals turning away from hiring foreign workers, because of the H-1B penalty now. The suspension of J-1 processing created backlogs. These visa bans that affect 75 countries on certain visas and 39 countries on others. You’ve got thousands of health care workers that are stuck outside the U.S. So what’s happening, really, is that hospitals and medical providers are just shutting down, and they’re cutting back services, and that means that there are less available services and resources for the same population and the same demand. People are waiting longer for doctor’s appointments. People are finding that they’re not able to get to the specialist that they need to get to in time. And so for us as practitioners, I think, we’re trying to navigate as best we can, but we’re just seeing a lot of people, employers that traditionally would rely on our services, give up and foreign workers looking to go elsewhere.
Rovner: I noticed during the annual residency match in March that it worked out, I think, fairly well for most graduating medical students. But the big sort of sore thumb that stuck out were international medical graduates. That’s going to impact the pipeline going forward, isn’t it?
Canero: From what I understand, it takes like seven to 15 years to get to that level, and we just don’t have the student body to meet the demand of residency positions. From my understanding, there’s a gap between American graduates and the demand for residents that’s usually filled by foreign workers. And if we don’t have those foreign workers, those residency positions just don’t get filled. And that becomes more expensive for hospitals, and that transfers to our medical bills.
Rovner: And people assume that, Oh well this doesn’t impact me. But it really impacts all patients, doesn’t it? And I would think particularly those in rural areas, which are less desirable for U.S.-born and -trained medical professionals and tend to be overrepresented by immigrants.
Canero: Yeah, I think a lot of the J-1 doctors and H-1B doctors are what facilitate, are working at, our veterans hospitals and our rural medical facilities. And what’s ending up happening is the very same people that this administration touts to support their interests are being forced to travel farther for specialists, right? If there isn’t an endocrinologist in your area, you may have to drive 100 miles to go see that specialist, and you may forgo necessary medical care because of the inconvenience or the cost. And I think that’s hitting at our health.
Rovner: So you’re on the board of Immigrants’ List, which is working to change things politically. What’s one change that could really make a big difference in what we’re starting to see in terms of immigration and the health care workforce?
Canero: Well, asking Congress to actually do something. It’s been a problem for decades. So I don’t really know, but I think there’s a couple of things, whether it’s just policymakers supporting our fight against some of these illegal policy changes in courts, organizations supporting us with amicus briefs. For example, there’s a lot of lawsuits challenging these visa bans and these adjudicative holds and the H-1B fine. The more support that the plaintiffs in the litigation get, the more likely we are to resolve that through the court system. And then I hope that there’s enough pressure from hospitals and organizations that have real dollars that impact these elected officials to get them to start seeing, Hey, we need to pass reasonable immigration reform to address some of the loopholes that this administration is using to cause chaos in the system, right? They’re able to do this because we have a gap. We allow them to terminate TPS. We don’t have a structure to ensure that a community that’s been on TPS for 20 years gets grandfathered into some sort of more stable visa. We don’t have a system that precludes the administration from just putting a hold or a visa ban on nationalities. So it’s something that Congress is going to have to step up and do something about.
Rovner: What worries you most about sort of what’s going on with the immigration system and health care? What keeps you up at night? Obviously you, I know you work on more than just health care.
Canero: I think my concern is that the American people aren’t seeing what’s happening, or they’re sort of turning a blind eye to it, and by the time it starts to actually impact them and they start asking, Wait, wait, wait. Why is this happening? I don’t understand, it’s going to be too late. Because it’s not hitting their pocket, because it’s not their suffering at this point, they’re not standing up and saying, Hey, this needs to stop, at the level that we need, opposition, to make it stop. And by the time it does hit their pocket and it does affect them directly, I think, it’ll be a little too late. I think people will be scared off from coming here, people that we needed will be gone, and to reverse the system is going to take decades.
Rovner: Michelle Canero, thanks again.
Canero: No, you’re very welcome. Thank you for your time.
Carey: OK, we’re back. Now it’s time for our extra-credit segment, and that’s where we each recognize a story we read this week and we think that you should read it, too. Don’t worry if you miss it. We’ll post the links in our show notes. Joanne, why don’t you start us off this week?
Kenen: Well, this is by Teddy Rosenbluth in The New York Times. The headline is “He Warned About the Dangers of A.I. If Only His Father Had Listened.” This is one of those stories where you know exactly how it’s going to end in the first paragraph, and yet it was so compellingly and beautifully written that you kept reading until the last word. It is, as the headline suggested, a young man who is an expert on AI and cognitive science named Ben Riley discovered that his father had been lying about a controllable, treatable form of leukemia. He had denied treatment, he’d refused treatment, he had ignored his oncologist because he was relying on AI. And as we all know, AI has its up moments and its down moments. And he was getting incorrect information, distrusted the diagnosis, refused treatment, getting sicker and sicker and sicker as the oncologist and the family got increasingly desperate. And the son, Ben Riley, had, like, skills. He knew how to find scientific evidence, and his father just would not believe it. And by the time his father finally consented to treatment, it was too late, and he did die. And his father was a neuroscientist, a retired neuroscientist, but he found a neuroscience rabbit hole.
Carey: That’s amazing. Anna, what’s your extra credit?
Edney: Mine, I’m highlighting a story that I wrote in Bloomberg called “Hormone Drugs Make $6.3 Billion Comeback After FDA Nixes Safety Warnings.” And this is, I wanted to dive into this policy that the FDA had implemented. The commissioner has long talked about and felt that perimenopausal and menopausal women were not getting access to the treatments that maybe they really needed, because there had been sort of this two-decade-old study that had showed there were some safety issues regarding breast cancer and cardiovascular disease, but the issue being that those studies had looked at older forms of the medication and also at women who were much older than those who might benefit from taking it. And so they, the agency, asked the companies to remove those warning labels, at least the strongest ones. And what we’ve seen, why — I wanted to dive into the numbers specifically. Bloomberg has some prescription data that was able to help me out here and just look at when this started rising. You could see that the prescriptions started going up around 2021. I feel like a lot of influencers, a lot of celebrities, were talking about this. And then in 2024 to 2025 when the FDA started talking about this, it really just goes, the prescription numbers just go straight up on the scale. And so there were about 32 million prescriptions written last year, which is a huge increase. And I just dove into some of this, some of the companies, what kind of drugs there are out there, and talked to some women who are benefiting but also, because of this pop, experiencing shortages, because the companies aren’t quite keeping up with the products.
Carey: Wow, that sounds like an outstanding deep dive. Thank you. Emmarie.
Huetteman: Yeah, my extra credit is from my colleague at KFF Health News who covers health technology. That’s Darius Tahir. The headline is “Your New Therapist: Chatty, Leaky, and Hardly Human.” The story looks at the proliferation of AI chatbot apps that offer mental health and emotional support, particularly the ones that market themselves as, quote-unquote, “therapy apps.” Darius counted 45 such apps in Apple’s App Store last month, and he uncovered in some cases that safety and privacy concerns existed, such as minimal age protections. Fifteen of the apps that he looked at said they could be downloaded by users who were only 4 years old. His story also explored the tension between the risks of sharing sensitive data and the interests of app developers and collecting that data for business purposes. It’s a good read. All right,
Carey: All right. Thanks so much. My extra credit is from Politico, and it’s written by Alice Miranda Olstein, and she’s a frequent guest here on What the Health? The headline is, quote, “‘A Crisis in the Making’: Nebraska Races To Impose Work Requirements on Medicaid,” close quote. The headline kind of says it all. Alice writes that Nebraska is racing to implement Medicaid work requirements by May 1, and that’s eight months ahead of the national deadline that was set by the One Big Beautiful Bill Act. Nebraska state officials plan to do this without hiring additional staff, even as other health departments in other states prepare to bring in dozens, if not hundreds, of new employees. Alice writes that advocates for people on Medicaid fear that this rush timeline and lack of new staff will cause many problems for Medicaid beneficiaries who are just trying to meet those new work requirements.
All right. That’s this week’s show. Thank you so much for listening. Thanks, as always, to our editor and panelist Emmarie Huetteman, to this week’s producer and engineer, Taylor Cook, and to my KFF colleague Richard Ho, who provided technical assistance. A reminder: What the Health? is now available on WAMU platforms, the NPR app, and wherever you get your podcasts, as well as, of course, kffhealthnews.org. Also, as always, you can email us with your comments or questions. We’re at whatthehealth@kff.org. Or you can find me on X, @maryagnescarey. Joanne, where can people find you these days?
Kenen: Bluesky and LinkedIn, @joannekenen.
Carey: OK. Anna?
Edney: Bluesky and LinkedIn and X, @annaedney.
Carey: And Emmarie.
Huetteman: You can find me on LinkedIn.
Carey: We’ll be back in your feed next week. Until then, be healthy.
Credits
Click here to find all our podcasts.
And subscribe to “What the Health? From KFF Health News” on Apple Podcasts, Spotify, the NPR app, YouTube, Pocket Casts, or wherever you listen to podcasts.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.This <a target="_blank" href="https://kffhealthnews.org/podcast/what-the-health-442-cdc-director-nominee-rfk-hearing-april-17-2026/">article</a> first appeared on <a target="_blank" href="https://kffhealthnews.org">KFF Health News</a> and is republished here under a <a target="_blank" href="https://creativecommons.org/licenses/by-nc-nd/4.0/">Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="https://kffhealthnews.org/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="https://kffhealthnews.org/?republication-pixel=true&post=2182989&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>This story also ran on CBS News. It can be republished for free.
According to new data from the Centers for Disease Control and Prevention, there were 3.6 million births in 2025, a 1% decline from 2024. The fertility rate dropped to 53.1 births per 1,000 women ages 15 to 44, down 23% since 2007.
The Trump administration has said it wants to reverse this trend. President Donald Trump has called for “a new baby boom,” and aides have solicited proposals from outside advocates and policy groups ranging from baby bonuses to expanded fertility planning. The administration is also proposing to reshape the federal government’s only dedicated family planning program: Title X.
For more than five decades, Title X has been geared — with bipartisan support — toward giving low-income women access to contraception, screening for sexually transmitted infections, and reproductive health care regardless of ability to pay. At its peak, the safety net program served more than 5 million patients a year. Six in 10 Title X clients have reported the program as their sole source of health care in a given year.
In early April, the Department of Health and Human Services invited nonprofit organizations to apply for Title X grants for fiscal year 2027, which begins in October. The 67-page Notice of Funding Opportunity included only one mention of contraception — describing it as overprescribed, associated with negative side effects, and part of a broader “overreliance on pharmaceutical and surgical treatments.”
The grant notification reshapes the program from its traditional public health intervention efforts to focus on fertility, family formation, and reproductive health conditions such as polycystic ovary syndrome, endometriosis, low testosterone, and erectile dysfunction.
While Title X will continue to help women “achieve healthy pregnancies,” the grant document does not explicitly reference preventing unintended pregnancies — a long-standing goal of the program.
Jessica Marcella, who oversaw the Title X program as a senior official in the Biden administration, said the new funding notice amounts to a wholesale redefinition of family planning.
“What we’re seeing is trying to use our nation’s family planning as a Trojan horse for an entirely different agenda,” Marcella said, noting that Trump has proposed eliminating Title X altogether.
Birth Rates and Fertility Trends
The administration is overhauling Title X in the context of declining birth rates. But researchers who study fertility trends say the decline is driven by forces that have little to do with contraception access and that restricting it is unlikely to produce more births.
The most important factors, according to demographer Alison Gemmill of UCLA, are timing-related. “Childbearing is increasingly delayed as part of a broader shift toward later adult milestones, including stable employment, leaving the parental home, and marriage,” she said.
Most American women, she said, still complete their childbearing years with an average of two children, suggesting a shift toward smaller families rather than an increase in childlessness.
“Having children has become more contingent and more planned,” she said.
Much of the decline since 2007 reflects women postponing births rather than forgoing them.
“The average number of babies women are having in their whole lives has not fallen. It’s still more than 2.0 for women aged 45,” said Philip Cohen, a professor of sociology at the University of Maryland.
Phillip Levine, an economist at Wellesley College, said the birth rate has declined due to shifts in how women approach work, leisure, and parenting. “Efforts to reverse those patterns would be more successful if they can make childbearing more desirable, not make it harder to prevent a pregnancy,” he said.
Asked about the role of contraception in reducing maternal mortality and how the new funding notice advances that goal, HHS press secretary Emily Hilliard said in a statement: “Applicants for the 2027 Title X funding cycle will be expected to align with the administration’s stated priorities in the released Notice of Funding Opportunity. HHS, under the leadership of Secretary Kennedy and President Trump, will continue to support policies that support life, family well-being, maternal health, and address the chronic disease epidemic. HHS remains focused on improving maternal outcomes and ensuring programs are administered consistent with applicable law.”
Marcella said the new funding notice is the product of two converging forces: the Make America Healthy Again movement, with its skepticism of conventional medicine and emphasis on lifestyle and behavioral interventions, and a pronatalist agenda that seeks to boost birth rates by steering policy toward family formation.
The document’s language reflects both: It repeatedly invokes “optimal health” and “chronic disease” while sidelining the contraceptive services that have defined Title X for half a century.
Clare Coleman, president and CEO of the National Family Planning & Reproductive Health Association, which represents health professionals focused on family planning, said tying Title X to birth-rate goals replaces individual decision-making with a government objective. The program “is designed to facilitate access to family planning services, including services to achieve and prevent pregnancy,” she said.
Title X’s New Focus
The administration’s changes have been welcomed on the right.
Emma Waters, a senior policy analyst at the conservative Heritage Foundation, who has advocated for what she calls “restorative reproductive medicine,” said the new funding notice reflects overdue attention to neglected aspects of women’s health.
“I was particularly encouraged to see language that spoke to the delays in diagnosis for conditions like endometriosis, the need for women to practically understand how their cycle and fertility works, and to ensure that real root-cause was promoted through Title X,” Waters said.
She described the notice as an expansion, not a narrowing, of the program’s mission: “I see this iteration of Title X as the fulfillment of its purpose. The goal was never just ‘more contraception’ but a wholesale empowerment of women to govern their own fertility.”
Waters also argued that untreated reproductive health problems may contribute to lower birth rates.
“One of the interesting aspects of this debate, and one that is often overlooked, is the degree to which painful and unaddressed reproductive health problems may suppress or create ambivalence around a woman’s desire to have kids,” she said, pointing to endometriosis.
An estimated 5% to 10% of women of reproductive age have endometriosis, and of those, 30%-50% experience infertility. Scientifically speaking, the relationship is an association, not a proven cause. Women aren’t screened for endometriosis if they don’t have symptoms, and the condition may be more prevalent than is recognized. Researchers still do not fully understand why some women with endometriosis struggle to conceive while others do not, and treating the disease does not reliably restore fertility.
Infertility rates in the U.S., meanwhile, have not risen. An analysis of federal survey data found them essentially flat between 1995 and 2019, even as the national birth rate fell sharply — a divergence that points away from untreated reproductive disease as an explanation.
Meanwhile, in February, the American College of Obstetricians and Gynecologists issued new clinical guidelines enabling earlier diagnosis of endometriosis without surgery, a step toward addressing the delays Waters described. But the first-line treatment ACOG recommends is hormonal therapy, part of the same category of care the funding notice dismisses as part of an “overreliance on pharmaceutical and surgical treatments.” The effect, reproductive health experts say, is a contradiction: Title X is now prioritizing diagnosis of endometriosis while deemphasizing the drugs clinicians use to treat it.
Treatments that have been shown to improve fertility in women with endometriosis, such as laparoscopic surgery and in vitro fertilization, are not covered by Title X. When President Richard Nixon signed Title X into law in 1970, he described it as a way to expand access to family planning services — helping women determine the number and spacing of their children by making contraception and related preventive care more widely available, particularly for those who could not afford it. Medicaid, not Title X, is the primary government health insurance program covering health care for low-income women, but, like many commercial insurance plans, it does not cover IVF.
Many of the conditions prioritized in the funding notice deserve attention, said Liz Romer, a former chief clinical adviser for the HHS Office of Population Affairs who helped write updated guidelines for the family planning program. But they fall outside the scope of what Title X can realistically provide.
“There’s not even enough funding to support the core premise of contraception,” Romer said. “And so, if you want to expand Title X funding, you can expand the scope, but you can’t move away from the foundation.”
The emergence of an anticontraception ideology within federal health policy is striking, she said, given how broadly the public supports access to birth control. Eight in 10 women of childbearing age surveyed by KFF in 2024 reported having used some form of contraception in the previous 12 months.
Laura Lindberg, director of the Concentration in Sexual and Reproductive Health, Rights and Justice at Rutgers School of Public Health, said, “If contraception is sidelined in Title X, it won’t just change language on paper but will show up as fewer options and more barriers for patients.” Funding could move away from providers who offer a full range of contraceptive care, she added, “toward organizations that are ideologically opposed to contraception and don’t deliver the same standard of health care services.”
The Stakes Are High
The United States already has one of the highest maternal mortality rates among wealthy nations — 17.9 deaths per 100,000 live births as of 2024. According to the CDC, 4 in 5 pregnancy-related deaths in the U.S. may be preventable. Medical research shows that pregnancy carries substantially higher risks of blood clots, stroke, and cardiovascular complications than hormonal contraception.
And since the Supreme Court’s Dobbs decision in 2022, which overturned the constitutional right to abortion established by Roe v. Wade, access to abortion has been significantly curtailed across much of the country. While national abortion numbers have risen, driven largely by telehealth and interstate access, research shows births have increased in states with bans, with an estimated 32,000 additional births annually, disproportionately among young women and women of color.
Dr. Christine Dehlendorf, who directs the Person-Centered Reproductive Health Program at the University of California-San Francisco, said “there is absolutely no evidence for any positive outcome of restricting access to contraception.” Restrictions would instead increase demand for abortion care and make it harder for women to prevent high-risk pregnancies.
Since Trump returned to office, more than a dozen Title X grantees have had their grants frozen, forcing some health centers to stop delivering services, lay off staff, or close. During the first Trump administration, regulatory changes led to a decline in Title X participation from more than 4 million patients to 1.5 million. The program grew slowly under the Biden administration, reaching about 3 million clients, before the current round of disruptions began.
The second Trump administration’s overhaul of the program, Marcella said, “directly undermines the public health intent of our nation’s family planning program and will potentially exclude millions of individuals from getting the care they have relied on for decades. It’s bad policy.”
This <a target="_blank" href="https://kffhealthnews.org/public-health/us-birth-rate-decline-title-x-family-planning-grants-contraception-pronatalist/">article</a> first appeared on <a target="_blank" href="https://kffhealthnews.org">KFF Health News</a> and is republished here under a <a target="_blank" href="https://creativecommons.org/licenses/by-nc-nd/4.0/">Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="https://kffhealthnews.org/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="https://kffhealthnews.org/?republication-pixel=true&post=2228147&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>Mayor Helena Moreno signed an executive order on April 7 that creates a task force to improve the New Orleans Recreation Development Commission. One of the task force’s duties will be to “consider and make recommendations regarding the costs and practicalities of implementing a program to assess and remediate safety and environmental concerns at NORDC facilities and playgrounds, including the existence of lead in soil” and other environmental issues, according to the order.
About a week before Moreno signed that order, Deputy Mayor of Health and Human Services Jennifer Avegno announced that city officials were working with the state’s congressional delegation to request $5 million in federal funds for the federal fiscal year that starts in October. That money would go toward testing and the possible cleanup of playgrounds with elevated levels of lead. She said her office is also reviewing past city records, working with the city’s in-house experts in its Planning Commission’s Brownfield Program, and reviewing Verite’s soil test results.
“We’re trying to figure out, with whatever pots of money we can get, how can we make a more sustained and meaningful impact than we have been able to in the past?” Avegno said during an April 1 panel discussion of Verite’s lead contamination investigation.
In the investigation published in February, Verite reporters tested more than 80 playgrounds for lead and documented unsafe levels of the toxic metal at just over half of them. Since then, parents across the city have called the New Orleans Recreation Development Commission, their elected officials, and other city offices seeking action.
But with the city in the midst of a budget crisis, parents and community groups in one neighborhood are taking action themselves. They are trying to raise $8,000 to hire a contractor to do extensive testing in the Bywater neighborhood’s Mickey Markey Playground, where Verite recorded lead samples that exceeded the federal hazard level of 200 parts per million — one sample registered at 403 parts per million.
“I’m aware of the city budget issues right now, and I’m also aware that fixing one playground in one neighborhood might not be a giant priority,” said Devin DeWulf, a father of two who lives in Bywater and founded the Krewe of Red Beans, a community organization helping with the fundraising.
Lead contamination persists in New Orleans soil, older buildings, and drinking water, posing a significant public health threat to children. Children under 6 can absorb the toxic metal more easily than adults, contaminating their blood and harming the long-term development of their brains and nervous systems.
There is no known safe exposure level for children or adults. In children, even trace amounts can result in behavioral problems and lower cognitive abilities. Chronic lead exposure for adults can increase the risk of heart problems and other health issues.
Beyond the effects on a single child or family, Avegno said, lead exposure has long-term implications, including its potential link to increases in violent crime, which makes the issue even more critical.
“We knew we had to exhaust every avenue,” she said.
Due to low rates of testing, it’s unclear how many children across New Orleans are exposed to lead. In 2023, just 17% of children were tested for lead poisoning in New Orleans, despite a state law that requires medical providers to test all children by age 1 and again by 2. Currently, the state Department of Health doesn’t have a mechanism for enforcing the law.
Public health researchers recommend parents avoid playgrounds with lead contamination because it can be difficult to prevent young children from placing dirt in their mouths or breathing in dust kicked up during play.
Vann Joines, a Bywater neighborhood resident who often takes his 2-year-old daughter to Mickey Markey Playground, is part of the group raising money to independently test the playground.
“It’s really important for us to be exceedingly mindful at public playgrounds and at public parks,” Joines said.
DeWulf and Joines said they anticipate the work will take a few years and hope to create a playbook that other neighborhoods can follow for their own playgrounds.
“We could create a how-to guide on how we could effectively do this in partnerships in the city,” Joines said.
On top of the $5 million the city is requesting for soil testing and possible remediation, Avegno said the city planned to apply for a grant to help address lead at early childhood education centers.
“Your story was amazing timing,” she told a Verite reporter.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.This <a target="_blank" href="https://kffhealthnews.org/public-health/lead-testing-new-orleans-playgrounds-investigation-cleanup/">article</a> first appeared on <a target="_blank" href="https://kffhealthnews.org">KFF Health News</a> and is republished here under a <a target="_blank" href="https://creativecommons.org/licenses/by-nc-nd/4.0/">Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="https://kffhealthnews.org/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
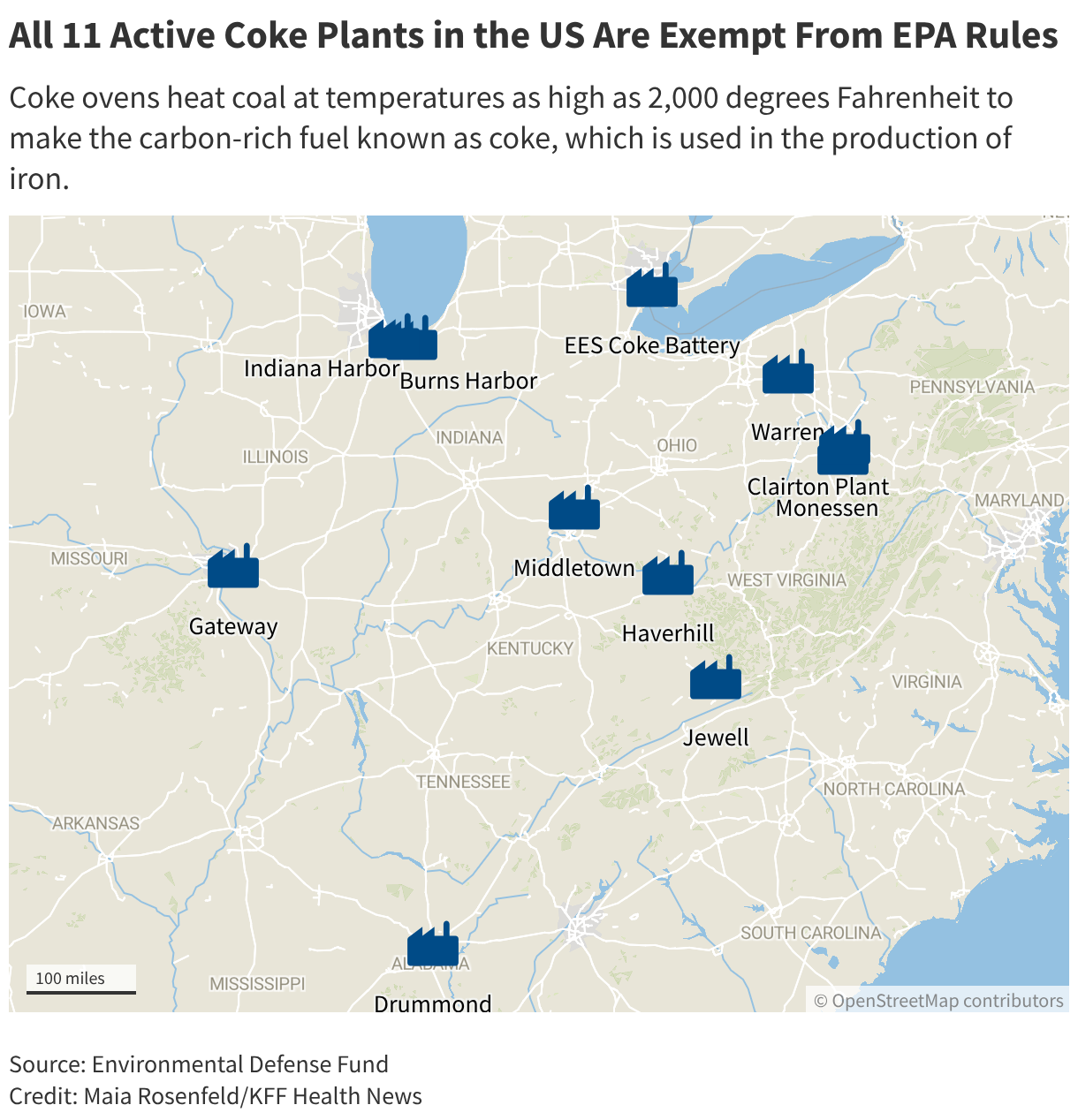
<img id="republication-tracker-tool-source" src="https://kffhealthnews.org/?republication-pixel=true&post=2181905&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>Researchers say the children at Clairton Elementary School about a mile away pay the price. They discovered the students there and at other elementary schools near major pollution sites in Pennsylvania had higher asthma rates than other children in the state.
Residents and environmental advocates saw reason for hope and relief in the form of a Biden administration rule designed to tamp down on coke oven plant pollution. But even before it took effect, President Donald Trump granted all 11 coke plants in the U.S. — including the one in Clairton — a two-year exemption from the standards.
Trump and Republicans have sought to align themselves with the Make America Healthy Again movement’s populist ideals, such as improving Americans’ food choices and reducing corporate harm to the environment. But the administration is ratcheting up its attacks on the very environmental protections that MAHA followers hold dear.
Taken together, these anti-environmental initiatives will lead to more pollution-related illnesses and higher health care spending, health researchers say. They could also have political ramifications, eroding MAHA’s support for GOP candidates in the November midterm elections if followers believe the party is more beholden to industry than to the movement’s agenda.
Only 1 in 5 American adults, including about a quarter of Republicans, support rolling back environmental regulations, according to a poll by the Energy Policy Institute at the University of Chicago and The Associated Press-NORC Center for Public Affairs Research.
Some MAHA supporters believe voters will support Republicans because the Trump administration is delivering on other goals important to the movement.
“MAHA has a pretty diverse set of policy goals, ranging from medical freedom to food and the environment,” said David Mansdoerfer, who served in Health and Human Services leadership during Trump’s first term. “In totality, the Trump administration has strongly delivered on much of the MAHA agenda.”
While MAHA voters have been upset at some of the administration’s actions that promote industry, it’s hard to know how that may play out in the midterms, said Christopher Bosso, a professor of public policy and politics at Northeastern University. Many were disillusioned by a Trump executive order they viewed as promoting glyphosate, which HHS Secretary Robert F. Kennedy Jr. has called poison.
“The glyphosate thing really ticks off a lot of them; they’re really upset,” Bosso said. “Kennedy said it was poison. If it is a poison, why aren’t we regulating it? That’s where the tension plays out.”
The situation with the Clairton coke plant and the others granted exemptions from regulations underscores the potential public health risks. Six of the 11 factories had “high priority” violations of the Clean Air Act as of last May, according to a KFF Health News analysis. Five coke oven plants logged major violations every quarter for at least three years straight.
“Poisoning continues to some of the most vulnerable residents of Allegheny County,” David Meckel, who had lived in nearby Glassport, Pennsylvania, said at a March 2025 county meeting about the coke plant.
Environmental Protection Agency spokesperson Brigit Hirsch said the president gave companies extra time because the technology needed to meet a new standard isn’t ready yet.
“Forcing plants to comply before the tools exist doesn’t make the air cleaner, it just shuts down facilities and kills jobs with nothing to show for it,” Hirsch said.
But environmental groups disagree that the plants were unable to comply at a reasonable cost, and they say the exemption from the EPA requirements shows the Trump administration is prioritizing the coal industry at the expense of public health.
“The Trump administration’s relentless actions to dismantle lifesaving environmental protections are a gut punch to the administration’s own promise to Make America Healthy Again,” said Cathleen Kelly, a senior fellow at the Center for American Progress, a liberal think tank.
Hard Times in Clairton
Sprawled across nearly 400 acres, the Clairton plant operates ovens in which coal is heated to as much as 2,000 degrees Fahrenheit to make up to 4.3 million tons annually of the carbon-rich fuel known as coke. The product is used in blast furnaces to produce iron.
It’s a dirty operation. The process leads to hazardous emissions of benzene, a carcinogen that the Centers for Disease Control and Prevention says can lead to anemia and leukemia, as well as sulfur dioxide, which can trigger severe asthma.
The Clairton operation has had repeated problems with its emissions and operations, including fatal explosions and excess releases of toxic chemicals. The plant has received more than $56 million in fines from the Allegheny County Health Department since 2022, stemming largely from a fire in 2018 that led to high emissions, and violated the Clean Air Act in each of the last 12 quarters, with the last compliance monitoring in July 2025, according to the EPA.
Nippon Steel Corp. last year acquired U.S. Steel, which now operates as a subsidiary. The company didn’t respond to an email seeking comment. U.S. Steel said it spends $100 million annually on environmental compliance at Clairton.
“Environmental stewardship is a core value at U. S. Steel, and we remain committed to the safety of our communities,” spokesperson Andrew Fulton said in a written statement.
Clairton was once bustling with movie theaters, a mix of grocery stores, and riverside parks, with a dance pavilion and a performing hot-air balloonist. But the decline of steel hit hard. The town’s population dwindled from more than 19,000 people in the mid-20th century to fewer than 6,000 as of 2024. Dozens of homes stood abandoned until they were razed and replaced with signs saying to keep out. The 1978 movie The Deer Hunter, which depicts a hardscrabble industrial town, is partly set there. Today, about 33% of residents live in poverty.

While the plant brings jobs and revenue, residents of the town and the surrounding areas have long complained about health problems they attribute to its emissions.
“My parents are gone. My mom had cancer, my dad,” Carla Beard-Owens, a Clairton resident, said at a 2025 County Council meeting. “I lost a lot of loved ones and seen other ones pass because of this mill.”
Pediatric allergist Deborah Gentile looked into asthma rates among 1,200 children who attended school near major pollution sites in the area — including students at Clairton Elementary School. They had nearly triple the national rate of asthma, with the highest rate among African American youth, according to the study she led.
“We were shocked,” she said. “It was double or triple what we expected. The people are proud of their industrial background. We need steel, but they’re not running a good enough operation.”
A follow-up study found children with asthma living near the coke plant had an 80% higher chance of missing school when sulfur dioxide pollution was elevated.
Allegheny County, which includes Clairton and Pittsburgh, is home to a number of industrial plants, and researchers have linked its air pollution to increased deaths, chronic heart disease, and adverse birth outcomes. It was ranked in the top 1% of counties in the nation for cancer risk from stationary industrial air pollutants in a 2018 EPA report.
Clairton has an age-adjusted cancer death rate of 170 per 100,000 people, higher than the broader county’s rate of 150 deaths per 100,000 people, based on a KFF Health News analysis of state and federal data.
The American Lung Association in 2025 gave the county an F rating for its particle pollution levels. PennEnvironment, an environmental group that was party to a settlement with U.S. Steel involving the Clairton plant, says the coke operation caused 1.1 million pounds of toxic releases in 2021, which amounted to 60% of all such releases in the county that year.
From 2020 through 2025, the Clairton plant racked up more in fines from Clean Air Act penalties than any other coke oven facility nationwide, costing U.S. Steel over $10 million, according to EPA facility reports.
“We are deeply concerned with exemptions, which allow air toxics to affect public health,” Allegheny County Health Department spokesperson Ronnie Das said in a statement.
The Clairton plant provides 1,200 manufacturing jobs and hundreds of millions of dollars in tax revenue to the area. The jobs help generate nearly $3 billion in annual economic output, according to estimates from the Pennsylvania Manufacturers’ Association.
Some community members and advocacy groups hoped air quality would improve after the coke plant was sold. Nippon Steel has pledged to upgrade facilities in the Monongahela River Valley.
Politics, Waivers, and Environmental Concerns
Under the Biden-era rule, coke plants were supposed to start meeting new limits on leaks from the lids and doors of ovens that heat coal. They would also have had to monitor for benzene at their property lines and take steps to lower emissions of the carcinogen if they exceeded certain levels. Compliance deadlines were set for July 2025.
The Trump administration, which has sought to revive the coal industry, intervened. Last year, it invited hundreds of industrial plants, including coke plants such as Clairton’s, to seek presidential waivers from nine separate rules issued in 2024 by the EPA.
Then Trump in November went further, granting all coke plants a two-year compliance break.
The reprieve was necessary, the EPA spokesperson Hirsch said, because the requirements would have meant extra costs for the industry when standards already in effect work “extremely well” at reducing pollution.
Hirsch also said the agency under Trump is protecting the environment, pointing to action the administration has taken to reduce long-lasting chemicals called PFAS, prevent lead poisoning, strengthen chemical safety, and protect Americans’ food and water supply.
“We are building a future where the next generation of Americans is the healthiest in our nation’s history, and they inherit the cleanest air, land and water in the world,” Hirsch said.
However, the administration has taken several steps that environmental advocates say weaken health protections.
The president’s executive order on glyphosate, an herbicide the World Health Organization has linked to cancer, which touched off a furor among MAHA enthusiasts who said they felt betrayed. The EPA has decided to stop considering the health-related economic benefits of reducing pollution when making policy decisions, instead focusing on the cost to industry of complying with rules. The agency also rescinded the legal and scientific basis that had long established greenhouse gases as dangerous to public health.
The actions have rankled some MAHA enthusiasts who counted on the administration to tackle chronic disease, especially among children. A petition to Trump on Change.org with more than 15,000 signatures called for the removal of EPA Administrator Lee Zeldin, citing deregulatory actions it said supported corporations over MAHA goals.
Some MAHA enthusiasts have sounded off on social media.
“No one should believe that MAHA is being upheld at the EPA at this point,” Kelly Ryerson, a leader of American Regeneration, which focuses on a conservation approach to farming, said Feb. 8 on X.
Alex Clark, host of a health and wellness podcast, also aired her concerns on X, saying “there is something really freaking spooky going on at the EPA and I refuse to let the American people be gaslit into thinking they’re upholding the MAHA agenda.”
“A significant number of people who supported Trump are worried these rollbacks are going to hurt their health,” said Max Burns, a Democratic strategist and the founder of the communications firm Third Degree Strategies. “The MAHA voters, especially women, are very sensitive to this. Republicans have put themselves in a bind.”
MAHA supporters shouldn’t be surprised by a Trump administration that doesn’t prioritize environmental protections over industry, because the president has always championed fossil fuels, said Kyle Kondik, managing editor of Sabato’s Crystal Ball, a nonpartisan election forecasting newsletter published by the University of Virginia Center for Politics.
The coke plant exemptions have disappointed some community members, environmental groups, and regulators concerned about public health and emissions.
Nearly 300,000 people live within 3 miles of the 11 active coke plants across the U.S., according to EPA data compiled by the Environmental Defense Fund.
Weakening environmental rules has helped boost Trump with the $91 billion U.S. coal industry. In February, mining industry executives and lobbyists gathered at the White House, greeting Trump with applause.
Coal miners, including some in white hard hats bedecked with American flags, presented him with a bronze-colored trophy emblazoned “The Undisputed Champion of Beautiful Clean Coal.”
At the event, Trump praised their work. “We love clean, beautiful coal,” he said.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.This <a target="_blank" href="https://kffhealthnews.org/public-health/clairton-pennsylvania-us-steel-make-america-healthy-again-maha-coal-coke/">article</a> first appeared on <a target="_blank" href="https://kffhealthnews.org">KFF Health News</a> and is republished here under a <a target="_blank" href="https://creativecommons.org/licenses/by-nc-nd/4.0/">Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="https://kffhealthnews.org/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="https://kffhealthnews.org/?republication-pixel=true&post=2178095&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>LISTEN: After a federal judge blocked the Trump administration’s efforts to pare down childhood vaccine recommendations, plenty of questions remain — like how annual vaccines for the flu will get approved. KFF Health News chief Washington correspondent Julie Rovner spoke with WAMU about how the decision is rippling through the public health system.
Big swings in federal vaccine policy are creating confusion for some parents and clinicians. A federal judge recently struck down Health and Human Services Secretary Robert F. Kennedy Jr.’s new, shortened list of recommended vaccines for all kids. But with the Trump administration likely to appeal, the situation is in flux. Meanwhile, cases of vaccine-preventable illnesses such as measles, mumps, and whooping cough continue to accumulate nationwide and in the Washington, D.C., area.
Julie Rovner, KFF Health News chief Washington correspondent and host of the podcast What The Health?, appeared on WAMU’s “Health Hub” on April 1 to break down what’s changed, what hasn’t, and what’s still unclear.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.This <a target="_blank" href="https://kffhealthnews.org/public-health/listen-wamu-health-hub-julie-rovner-explains-acip-vaccine-schedule-court-judge/">article</a> first appeared on <a target="_blank" href="https://kffhealthnews.org">KFF Health News</a> and is republished here under a <a target="_blank" href="https://creativecommons.org/licenses/by-nc-nd/4.0/">Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="https://kffhealthnews.org/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="https://kffhealthnews.org/?republication-pixel=true&post=2177579&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>The CDC withheld the data for months as a team hit hard by mass layoffs and resignations sorted through the information. But now that scientists at the agency have posted their first batch of whole measles genomes — the genetic blueprint of the viruses — the rest should “start flowing more smoothly at a more rapid cadence,” said Kristian Andersen, an evolutionary virologist at the Scripps Research Institute who isn’t involved with the CDC’s effort but is following it.
The CDC did not answer queries from KFF Health News on its timeline for publishing measles data or analyses. However, once all the data is public, researchers can run quick initial analyses that will signal whether outbreaks across the U.S. last year resulted from the continuous spread of the disease between states, rather than separate introductions from abroad. If there was continuous transmission for a year, that means the U.S. has lost its status as a country that has eliminated measles. That status, which the U.S. has held since 2000, reflects a country’s vaccination rates: Two doses of the measles-mumps-rubella vaccine prevent most infections and so stop outbreaks from growing.
More careful analyses take weeks.
“We should see a report in April,” Andersen said, “assuming no political interference.”
This is the first time that the U.S. has applied sophisticated genomic techniques to measles, which largely disappeared from the country a quarter-century ago because of broad vaccine uptake.
Declining vaccination rates, misinformation, and the Trump administration’s budget cuts and lagging response to outbreaks have fueled a resurgence of the disease. With at least 2,285 cases in 44 states, 2025 was the worst year for measles in more than three decades. This year is on track to surpass that, with 1,575 cases as of late March.
While welcoming the science, researchers say the government’s top priority should be to stop the virus from spreading.
“I think it’s incredibly important to do whole genome sequencing for outbreaks,” Andersen said, “but we shouldn’t need to do this for measles in the first place, because we have an extremely effective and safe vaccine.”
“That we’re even talking about this is nuts,” he added.
Health and Human Services Secretary Robert F. Kennedy Jr. and other government officials should sound an alarm about measles’ comeback and launch nationwide vaccine campaigns, said Rekha Lakshmanan, executive director of The Immunization Partnership, a nonprofit in Houston that advocates for vaccine access.
“I applaud the science,” she said, “but the more urgent need is to get measles under control as quickly as possible.”

Top officials have instead downplayed the seriousness of the disease, and false notions about vaccines have been granted new life in Kennedy’s CDC. This includes abrupt changes to vaccine information on CDC websites that medical associations say aren’t based on evidence and endanger lives.
Kennedy continues to promote unproven remedies that could mislead parents into believing that they can avoid vaccines without consequence. On the Joe Rogan Experience podcast in late February, Kennedy spoke at length about measures to improve America’s health but didn’t mention vaccines. He said preventive measures could entail “holistic medicine, or take vitamins, or take vitamin D, which is, as you know, it’s kind of miraculous.”
“The risk of measles remains low for most of the United States,” HHS spokesperson Emily Hilliard wrote. “CDC has made $8.5 million available to address measles response activities in 7 jurisdictions experiencing outbreaks,” she wrote. “The CDC, HHS principles, and the Secretary have been vocal that the MMR vaccine is the best way to protect yourself against measles.”
1,000 Genomes
In December, the CDC enlisted the help of one of the country’s leading centers for virus sequencing, the Broad Institute in Cambridge, Massachusetts. Major outbreaks in Texas, Utah, and South Carolina had been fueled by the same type of measles virus, labeled D8-9171. But since that type also circulates in Canada and Mexico, researchers need more data to discern whether it spread among states or entered the U.S. multiple times.
Whole genome sequencing provides that information because viruses evolve over time. The measles virus acquires a mutation every two to four transmissions between people, said Bronwyn MacInnis, director of pathogen surveillance at the Broad.
“There is enough signal in this data to tease apart questions at hand,” MacInnis said, “the main one being sustained transmission within this country.”
MacInnis’ team worked overtime to sequence the entire genomes of inactivated measles viruses that had been collected from states in 2025 and 2026.
“We’ve done about 1,000 samples and delivered the genome data back to the CDC,” sending it on a rolling basis since December, MacInnis said. “This is the CDC’s data to publish.”
The CDC didn’t post a single one of those genomes until late March, when eight appeared on a public database hosted by the National Center for Biotechnology Information. By April 1, an additional 154 had gone online.
“It should be on NCBI within a couple of weeks of being produced,” Andersen said, “and certainly not take longer than a month when you have an active outbreak.”
Genomic data holds clues about how outbreaks start and spread. It allows researchers to develop tests, treatments, and vaccines — and detect variants that might evade them.
Such data was critical in the covid pandemic. Chinese and Australian scientists posted the first SARS-CoV-2 genome online on Jan. 10, 2020, within a week of sequencing it. “It definitely shouldn’t take the CDC months,” said Eddie Holmes, the Australian virologist who helped publish the first coronavirus sequence.
One reason for the delay is that the CDC’s measles lab has been sorely understaffed amid mass layoffs and other turmoil at the agency over the past year, a CDC scientist told KFF Health News. Another reason, the researcher added, is a learning curve: The CDC and health departments haven’t needed to sequence hundreds of whole measles genomes before now. (KFF Health News agreed not to identify the scientist, who feared retaliation.)
In contrast with the CDC, the Utah Public Health Lab has shared measles genomes rapidly. Most of some 970 measles genomes posted online since Jan. 1, 2025, were sequenced by the state, hailing from Utah, Arizona, South Carolina, and other states willing to share them.
“We’ve only got a handful of samples from Texas that were collected kind of in the middle of their outbreak,” said Kelly Oakeson, a genomics researcher at the Utah Department of Health and Human Services. The genomes of the Texas and Utah measles viruses are similar but distinct, Oakeson said, meaning that intermediate versions of the virus are missing.
If the genetic code of viruses collected late in the Texas outbreak are a closer match to those from Utah’s, that will suggest that spread was continuous and the country has lost its measles-free status. The hundreds of genome sequences still sitting at the CDC probably hold the answer.
Waiting on the CDC
The CDC expected to finish its analysis before April, said Daniel Salas, executive manager of the immunization program at the Pan American Health Organization, which works with the World Health Organization. That’s when PAHO was slated to evaluate the United States’ measles status.
He said PAHO delayed its evaluation until the organization’s annual meeting in November, partly because the CDC needed more time to do the genomic analysis and partly because the measles status of Mexico, Bolivia, and other countries is also under review, and holding staggered meetings for each country is inefficient.
The U.S. is the only country using whole genome sequencing to answer the elimination question, Salas said. Typically, countries classify measles viruses according to a tiny snippet of genes, then assume that large outbreaks caused by the same type are linked. Whole genomes provide a more accurate view.
“If the U.S. can fill in the blanks with genomic data, that’s a sort of breakthrough,” Salas said. “That doesn’t mean other countries are going to be able to pull off this kind of analysis,” he added. “It takes a lot of specialized knowledge and resources.”
Equipment to sequence and analyze genomes costs upward of $100,000, and the cost to process each sample, including paying the researchers involved, typically ranges from $100 to $500 per sequence.
“I’m pro-science, but we shouldn’t have to do this,” said Theresa McCarthy Flynn, president of the North Carolina Pediatrics Society. “We don’t have to have a measles epidemic.”
Flynn said she regularly fields questions from parents concerned by misinformation spread by Kennedy and anti-vaccine groups, including the one he founded before joining the Trump administration. Parents have also pointed to changes in the CDC’s recommendations and to its websites that are at odds with the scientific consensus.
Before Kennedy took the helm, a CDC website said “Vaccines do not cause autism” in prominent type, and listed several large studies in premier scientific journals that refuted a link between vaccines and developmental disorders.
Last year, the website shifted to saying, “Studies supporting a link have been ignored by health authorities.” The high-quality studies were replaced with a report from a single investigator who has ties to anti-vaccine groups. In an email to KFF Health News, HHS spokesperson Hilliard echoed the altered website’s claims about vaccines, disregarding extensive studies on the topic.
Flynn, of the pediatrics association, said, “The CDC itself is spreading misinformation about vaccines. I cannot overstate the seriousness of this.”
Although the acting director of the CDC, Jay Bhattacharya, says vaccines are the best way to prevent measles, he too has undermined vaccine policy. He said the controversial January decision to reduce the number of vaccines recommended to children was based on “gold standard science.” In fact, the new schedule makes the U.S. an outlier among peer nations. Hilliard wrote that the updated schedule was “aligning U.S. guidance with international norms.”
A federal court temporarily invalidated the change last month in a lawsuit brought by the American Academy of Pediatrics and other groups.
Bhattacharya hasn’t held briefings with the public or the press on the surge of measles this year or activated the CDC’s emergency capabilities.
“Normally, we’d have a big push to get vaccination rates up in areas where it’s low. We’d do a big social media push, put out ads on getting vaccinated,” said another CDC scientist whom KFF Health News agreed not to identify, because of fears of retaliation. “People at the CDC want to do this, but political leadership at the agency has not allowed the CDC to do it.”
Further, the Trump administration’s cuts and delays to public health funds have made it hard for local health officials to protect communities. Philip Huang, director at Dallas County Health and Human Services in Texas, said the department lost over $4 million when the administration clawed back about $11 billion from health departments early last year as a measles outbreak surged in the state.
“We lost 27 staff and had to cancel over 20 of our community vaccination efforts, including to schools identified as having low vaccination rates,” he said. “There are simultaneous attacks on immunizations that are making our jobs harder.”
This <a target="_blank" href="https://kffhealthnews.org/public-health/measles-genome-cdc-data-elimination-status-outbreaks-rfk/">article</a> first appeared on <a target="_blank" href="https://kffhealthnews.org">KFF Health News</a> and is republished here under a <a target="_blank" href="https://creativecommons.org/licenses/by-nc-nd/4.0/">Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="https://kffhealthnews.org/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="https://kffhealthnews.org/?republication-pixel=true&post=2177574&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>According to a recording obtained by KFF Health News, Bhattacharya at one point suggested to CDC staff that Trump could name a new leader for the agency as soon as Thursday. “But if not, I don’t think much will change,” he said.
Though his official position as acting director was set to expire Wednesday, Bhattacharya will continue to lead the agency until the top spot is filled. Meanwhile, news outlets including Axios and The Washington Post reported that the administration was postponing filling the permanent director job amid the challenges of gaining Senate confirmation and other political pressures.
Bhattacharya opened the meeting by acknowledging the struggles the beleaguered agency has gone through over the past year. Workers faced waves of job losses, and a gunman attacked the CDC’s Atlanta campus in August, killing a police officer and causing significant property damage. “I want to acknowledge very honestly that I know that it has been such a difficult year for the CDC and for every single one of you here,” Bhattacharya said.
He said the agency has begun to fill its leadership gaps. During his first meeting with the agency’s top leaders, he said, “I noticed almost every single one of them is acting.”
“We’ve made progress in filling key roles across the agency,” he said. “Leadership stability is essential to delivering our mission.”
The aim, he said, is to leave the agency in “a solid, secure place” so it can do its work “without so much of the turmoil that we’ve seen the last year.”
Bhattacharya invited questions from the CDC staffers, who repeatedly asked about staffing losses, morale, and their job security, as well as Trump’s decision to withdraw from the World Health Organization.
“The politics of WHO withdrawal are above my pay grade,” Bhattacharya said. “What I do know is that without the CDC, the world will be in much worse health.”
Workforce Concerns
One employee told Bhattacharya the agency had lost a “huge amount” of “internal capacity and expertise in the past year” and it “continues to be very challenging for staff to do their jobs,” adding that “certain conditions are a bit demoralizing.”
The CDC can “function without leaders,” another speaker said. “We function without directors. And this entire team will make CDC run without you if you’re not here.”
Schedule F, an effort to reclassify certain federal employees in policy-related roles and reduce their civil service protections, drew some of the strongest statements from the staff. While it’s not fully implemented, the policy could make it easier for Trump to fire thousands of federal workers.
“What’s scaring the hell out of us right now is Schedule F,” an employee said. “We are terrified that ‘at will’ means you’re gone, you’re not here, you’re fired.”
“The Schedule F fight’s above my level,” Bhattacharya replied. He said his focus is on making sure the “work is supported.”
He said the agency should seek to “depoliticize what we do fundamentally” so that “every American sees us as working for their benefit.”
“When I say ‘depoliticize,’ I don’t mean you can’t say the hard or talk about the hard things,” he added. “I mean that you’re free to talk about the hard things without fear that you’re gonna be retaliated against.”
On hiring and operations, he pointed to ongoing efforts but acknowledged delays. The Department of Health and Human Services, which oversees the CDC, is “moving at the speed of bureaucracy,” he said, adding that he’s trying his best. “We have to move past the last year, and I think we now have an opportunity really to do that.”
Vaccine Policy
On vaccines, Bhattacharya said one of the first things he did in his role as acting CDC director was to record a video “strongly encouraging parents to vaccinate their kids from measles.”
He said rebuilding trust requires engagement. That means working with communities without denigrating them, and respecting how “they think and their values,” he said.
Bhattacharya said he would like the NIH and CDC to coordinate more, particularly on HIV prevention. He described his approach as “an implementation science strategy so that we can use these two pieces of the HIV tool kit to actually end the HIV pandemic.”
The search for a permanent CDC director is being led by HHS officials on behalf of the White House and Health and Human Services Secretary Robert F. Kennedy Jr.
Bhattacharya said he’s friends with Kennedy and called “the caricature of him that I’ve seen in the press” unfair. Kennedy “really does have a deep desire to make America healthy,” he said.
For now, Bhattacharya said, he expects to stay in place at the CDC, as “either acting director or acting in the capacity of the director, whatever the heck that means.”
He joked about the ambiguity: “It’s like an Office episode, you know?”
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.This <a target="_blank" href="https://kffhealthnews.org/public-health/cdc-jay-bhattacharya-acting-director-search-nomination-staff-cuts-morale/">article</a> first appeared on <a target="_blank" href="https://kffhealthnews.org">KFF Health News</a> and is republished here under a <a target="_blank" href="https://creativecommons.org/licenses/by-nc-nd/4.0/">Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="https://kffhealthnews.org/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="https://kffhealthnews.org/?republication-pixel=true&post=2173895&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>On the coffee table at her home in Atlanta, Sarah Boim has a pile of documents from her old job at the Centers for Disease Control and Prevention. They are printouts of her employment records.
Boim lost her job in the first big wave of CDC firings — more than 1,000 people were suddenly let go last February.
“This is the termination letter. I also printed off my performance review from 2024,” she said. “I knew I wouldn’t have access to it, and everything was so chaotic that I needed proof of what was happening.”
Boim worked in the National Center for Environmental Health/Agency for Toxic Substances and Disease Registry, handling communications about radon, substances known as forever chemicals, lead poisoning, and other health threats.
Rereading her termination letter, she still can’t believe what it says.
“The agency finds you are not fit for continued employment because your ability, knowledge, and skills do not fit the agency’s current needs, and your performance has not been adequate to justify further employment at the agency,” the emailed letter reads.
“And that floored me,” Boim said, “because my performance was rated outstanding, and I even got a raise. It was just deeply insulting. So I was more upset than I think I was prepared to be.”
The Trump administration later brought back some of the workers who were fired in the first round, but it has also cut more staff and funding.
The CDC has been without a permanent director for more than six months. Recently the Trump administration made Jay Bhattacharya the CDC’s interim director, while he also runs the National Institutes of Health.
The leadership uncertainty comes amid a year of disruption and dismissals at the Atlanta-based institution, from which more than 3,000 public health workers are now gone. That includes staffers the Trump administration terminated and workers who accepted early retirement.
Ripple effects of the turmoil are still hitting the Atlanta region.
By the end of 2025, the CDC had lost roughly a quarter of its workforce.

Boim now works as a contractor in the health field, while also working a non-health-related freelance job. But she mourns the cuts at the CDC, and how the loss of expertise and resources will trickle down to communities. A significant portion of CDC funding goes directly to states and local public health departments.
“It will cause generational harm, which always makes me tear up,” Boim said. “The harm that’s going to come to people that don’t even know what CDC was protecting them from.”
“But for Atlanta, there’s a lot of us; there are thousands of CDC employees that live here,” she added. “We are your friends, your neighbors, your family, and — with the lost income — it has an impact on local businesses also.”
At the SriThai restaurant across the street from the main CDC campus, more than a third of the customers are CDC employees, said manager Nathan Chanthavong.
The restaurant saw a “small dip” in business in 2025 after the mass firings, and also during the government shutdown, he said.

“Typically, we would get a catering order for the CDC. We saw it less, less, and less. It’s not a really big impact, but catering is a big order; it is a lot of money,” he said. “So it does affect us.”
The CDC falls under the purview of the Department of Health and Human Services.
“HHS under the Biden administration became a bloated bureaucracy, growing its budget by 38% and its workforce by 17%,” HHS spokesperson Andrew Nixon said of the cuts and attrition. “The Department continues to close wasteful and duplicative entities, including those that are at odds with the Trump administration’s Make America Healthy Again agenda.”
Since the mass firings began, former CDC workers and their supporters have protested outside the agency’s main entrance every Tuesday during the afternoon rush hour.
On a recent Tuesday, a bigger crowd than usual — about 75 people — lined up along the sidewalk. It had been a year since the first massive cuts, which occurred in mid-February 2025. CDC workers dubbed it the “Valentine’s Day massacre.”
Protesters waved handmade signs with slogans such as “We love CDC workers” and “Save Public Health.” Passing drivers honked in solidarity.
Among the protesters was Ben McKenzie, who is still employed as a CDC researcher.
“It’s been heartbreaking to see so many talented, able colleagues be forced out or leave,” he said.

Current employees also need support, he said, especially after a man opened fire on CDC buildings last summer. The gunman killed DeKalb County police officer David Rose before killing himself.
“I think we’ve all felt the emotional impact of being targets,” McKenzie said. “Right now, to work at CDC is in a lot of ways to be a target.”
Multiple CDC employees told KFF Health News and NPR the federal government has yet to fully fix the damage to the windows and buildings hit in last year’s shooting.

McKenzie helps run a mutual aid group, one of several that have sprung up in Atlanta. He said the group has distributed more than $200,000 to help former CDC workers with rent and other needs.
This article is from a partnership with WABE and NPR.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.This <a target="_blank" href="https://kffhealthnews.org/public-health/cdc-atlanta-public-health-one-year-later-firings-shooting-morale/">article</a> first appeared on <a target="_blank" href="https://kffhealthnews.org">KFF Health News</a> and is republished here under a <a target="_blank" href="https://creativecommons.org/licenses/by-nc-nd/4.0/">Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="https://kffhealthnews.org/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="https://kffhealthnews.org/?republication-pixel=true&post=2171927&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>
KFF Health News senior correspondent Renuka Rayasam discussed the KFF Health News series “Priced Out,” which focuses on the health insurance crisis, on An Arm and a Leg on March 19.
- Click here to hear Rayasam on An Arm and a Leg (starts at 21:03).
- Read Rayasam’s “When Health Insurance Costs More Than the Mortgage.”
KFF Health News rural health reporter Andrew Jones discussed the spread of measles across the Carolinas on WUNC’s Due South on March 17.
- Click here to hear Andrew Jones on Due South.
- Read Jones’ “Hospitals Fighting Measles Confront a Challenge: Few Doctors Have Seen It Before.”
Céline Gounder, KFF Health News’ editor-at-large for public health, discussed on CBS News 24/7’s The Daily Report on March 16 how U.S. hospitals and insurers are turning to AI to settle disputes over medical claims and payments. On March 17, she outlined the court ruling blocking the Trump administration’s vaccine policy changes for children on CBS News’ CBS Mornings. Gounder also discussed Susie Wiles’ decision to stay on as White House chief of staff amid breast cancer treatment on CBS News 24/7’s The Takeout on March 16.
- Click here to watch Gounder discuss hospitals, insurers, and AI on The Daily Report.
- Click here to watch Gounder discuss vaccine policy changes for children on CBS Mornings.
- Click here to watch Gounder discuss White House chief of staff Susie Wiles on CBS Mornings.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
This <a target="_blank" href="https://kffhealthnews.org/on-air/on-air-march-21-2026-insurance-prices-measles-spread-ai-vaccine-ruling-susie-wiles/">article</a> first appeared on <a target="_blank" href="https://kffhealthnews.org">KFF Health News</a> and is republished here under a <a target="_blank" href="https://creativecommons.org/licenses/by-nc-nd/4.0/">Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License</a>.<img src="https://kffhealthnews.org/wp-content/uploads/sites/8/2023/04/kffhealthnews-icon.png?w=150" style="width:1em;height:1em;margin-left:10px;">
<img id="republication-tracker-tool-source" src="https://kffhealthnews.org/?republication-pixel=true&post=2171531&ga4=G-J74WWTKFM0" style="width:1px;height:1px;">]]>